Research Article - (2016) Volume 0, Issue 0
Objective: Few studies have described the complications leading to transfemoral amputation after total knee arthroplasty. The aim of this study was to demonstrate which long term prosthesis-related complications can lead to the loss of a limb after knee joint replacement and to provide clinical guidance regarding the situations that generate an increased likelihood of a patient requiring above knee amputation after total knee arthroplasty. Methods: All patients who received above knee amputations between 2005 and 2015 at our clinic due to prosthesis-related complications after total knee arthroplasty were included in this retrospective study. We analyzed the frequencies of various reasons for above knee amputation as well as their influence on the decision to amputate. Results: Sixteen patients received a transfemoral amputation after total knee arthroplasty at our clinic during the study period. Joint infection was the principal reason for above knee amputation in all patients, and at least two additional factors that influenced the decision to amputate were present in each presented case. Conclusions: The indication leading to transfemoral amputation after total knee arthroplasty is always multifactorial. An infection is present in most cases as the main contributing factor and is usually accompanied by at least two other factors. In some cases of recurrent persistent periprothetic joint infections, transfemoral amputation remains the only salvage procedure in order to control the infection, and in some cases, it is a life-saving procedure.
Keywords: Knee joint replacement; Total knee arthroplasty; Joint infection
Total knee arthroplasty is the second most common joint replacement operation performed worldwide. In 2009 Germany had most knee replacement surgeries among the OECD countries with 213 per 100000 population and has remained among the top five in the following years [1-3]. According to national arthroplasty registries, the number of implanted knee endoprostheses each year is continuously increasing [4]. For example, by the year 2030, the number of primary total knee arthroplasty operations performed in the US is expected to increase to 3.4 million surgeries per year, compared to 600,000 total knee replacements performed in 2010 [5]. The usual lifetime of an endoprosthetic knee replacement lies between 10-25 years, which is dependent on diverse factors such as body weight, gender and the age of the patient [6-8]. The lifespan of an endoprosthetic knee replacement can be shortened if complications occur. These complications can be instability (10-20% of all knee revision surgeries), stiffness (1.3% prevalence), infections (25-43% of all knee revision surgeries), aseptic loosening (31-55% of all knee revision surgeries), periprosthetic fractures (5.6% of all revision surgeries) or even atypical implantations [9-11]. If complications occur, an untimely exchange of the prosthesis may be needed with infections being the leading cause for revision surgery after total knee arthroplasty [12,13]. Treatment options include irrigation and debridement with exchange of modular components or removal and reimplantation in a single-stage or two-stage revision, with the two-stage revision and temporary placement of an intraarticular antibiotic-loaded cement spacer becoming the gold standard [14]. In cases of recurrent persistent periprosthetic joint infections, salvage procedures are required; complete eradication of the infection can only be achieved by removal of all components and through knee-fusion (arthrodesis) or above knee amputation [14-18].
Most publications on transfemoral amputation after total knee arthroplasty are case reports [19-24] or small case series [25-28], and only three studies have included more than ten patients [29-31]. Only two publications have reported a prevalence (0.14-0.31%) of above knee amputation after total knee arthroplasty [30,32].
As the overall numbers of endoprosthetic replacements of the knee are continuously rising, the overall number of complications will also increase. Problematic cases of uncontrollable infections will also lead to an increasing number of transfemoral amputations after total knee arthroplasty. Therefore, a closer look may be needed to focus on the indications leading to above knee amputation after total knee arthroplasty. Hence, the aim of the present study was to investigate which prosthesis-related reasons influenced the decision to amputate after total knee arthroplasty.
Patients with an endoprosthetic knee replacement who were treated with a transfemoral amputation of the same leg at any time during the postoperative course between 2005 and 2015 were included into this study. It was a retrospective single center study. The indications for all prosthesis-related above knee amputations from the past ten years were reviewed and analyzed. All of the factors that influenced the decision to amputate were determined and studied.
To obtain our study group, we requested patient information from the controlling department of our hospital, where records of all diagnoses and procedures are maintained. From 2005 to 2015, all patients with potential prosthesis-related indications for above knee amputation were identified according to the International Classification of Procedures in Medicine (ICPM) number 5-864.5, which has typically been used to code operations involving above knee amputation. All of the identified patient files and x-rays were reviewed. Any patients who had undergone above knee amputation for nonprosthesis- related reasons were excluded (vascular diseases, tumors and infections without prostheses) because, in those cases, the above knee amputations were not related to knee prosthesis implantation (Figure 1).
Figure 1: Study population.
The following data were collected from the files of the remaining patients: baseline data, such as gender and age at time of primary knee joint arthroplasty; location and type of primary knee prosthesis implantation; date and reason for the first related operation following knee arthroplasty and number of operations after knee arthroplasty prior to amputation; preoperative body mass index (BMI); amount and type of concomitant diseases; amount and type of drugs administered prior to the amputation and duration of the amputation operation.
An infection was defined to be present if a preoperative puncture of the knee joint and direct microscopy by a microbiologist revealed intra articular bacteria, if intraoperative swabs revealed growth of the same bacteria in at least 2 out of 5 samples or if the patient had signs of infection in his/her blood (elevated C-reactive protein level or leukocytosis) with clinical signs of infection (rubor, tumor, dolor, calor, functio laesa). Periprosthetic infections were classified according to criteria described by Tsukayama [33].
Other factors that influenced the decision to amputate were determined from the antibiograms of the obtained bacteria, histopathological results of the amputated leg, operative protocols, patient files, x-rays, computed tomography (CT) scans, magnet resonance imaging (MRI) and photographs. The antibiograms were evaluated by a microbiologist, and the histopathological results were evaluated by a pathologist. The x-rays were independently evaluated by a radiologist and an orthopedic surgeon, and the CT scans and MRIs were evaluated by a radiologist. Sepsis was defined according to the criteria determined by the 2001 International Sepsis Definitions Conference [34].
Consent and ethical approval
All patients gave informed consent prior being included into the study. All procedures involving human participants were in accordance with the 1964 Helsinki declaration and its later amendments. The study was approved by the Research Ethics Committee (number 4/6/15).
Statistical analysis
For statistical evaluation, the software StatSoft, Inc. (2014) STATISTICA for Windows (Software-System for Data-analysis), Version 12.0 (www.statsoft.com) was used. The average, standard deviation (SD), median and range were calculated for all data.
Sample size
Sixty-six cases of above knee amputation were identified for which all patient files and x-rays were analyzed. This analysis led to the exclusion of 50 cases because the above knee amputations in these patients were performed due to a tumor, a vascular disease or an infection in the absence of a knee prosthesis.
Patient baseline characteristics
Sixteen patients (8 men and 8 women) were included for further analysis. At the time of total knee arthroplasty, the average age of the patients was 66.9 (SD ± 10.6 years; median 68.1 years; range 43.5- 82.4 years). The indication for total knee arthroplasty was primary osteoarthritis of the knee in all cases. Three patients had undergone primary prosthesis implantations at our institution, while the other 13 patients were referrals from other hospitals after prosthesis implantation. One patient had undergone a semi-constrained total knee arthroplasty, two patients had undergone a constrained total knee arthroplasty and 13 patients had undergone a surface total knee arthroplasty. All prostheses were cemented, except for one surface total knee arthroplasty. The average time from the primary implantation of the prosthesis to the first revision surgery was 63.7 months (SD ± 75.3 months; median 34.8 months; range 0.7-221.4 months). The reasons for the first revision surgery were infection in 14 cases and aseptic loosening and periprosthetic fracture in one case each. The average number of operations prior to above knee amputation was 7.8 (SD ± 13.0; median 4.5; range 0-55).
At the time of amputation, the average BMI of the patients was 29.7 (SD ± 9.7; median 25.4; range 21.5-58.8). The patients had an average of 7.8 concomitant diseases (SD ± 4.8; median 6.0; range 3.0-19.0). Two patients had rheumatoid arthritis. The patients were administered an average of 9.8 drugs (SD ± 4.9; median 9.0; range 1-22). Three patients were administered immunosuppressive drugs, and five patients were administered anticoagulation drugs. The average time from primary implantation to amputation was 95.7 months (SD ± 71.5 months; median 87.1 months; range 3.1-221.6 months). The average duration of the amputation operation was 95.3 minutes (SD ± 32.3 minutes; median 89.5 minutes; range 35.0-146.0 minutes).
Indications for prosthesis-related above knee amputations
In all cases, the indication to amputate was multi-factorial, and the average number of factors involved was 4.4 (SD ± 1.4; median 4.0; range 3.0-7.0) (Supplementary Table 1).
Infections
In all 16 patients, an intraarticular infection was present. According to the criteria described by Tsukayama, 8 infections were late and 8 infections were hematogenous. The infections were most commonly caused by Staphylococcus aureus (12 patients), followed by Staphylococcus epidermidis (8 patients). The infection was complicated in every case due to the presence of at least one of the following factors:
• Multiple bacteria (11 patients)
• Adjacent osteitis (9 patients)
• Multi-drug resistance (8 patients)
• Concomitant sepsis (8 patients).
Other observations related to infection included a pyarthros in 4 cases and an adjacent soft tissue abscess in 3 cases, as described in the operative protocols. Additionally, 1 patient had necrotizing fasciitis.
Fractures
Three patients had periprosthetic fractures. In 1 case, the periprosthetic fracture was a fatigue fracture of the tibial plateau, and in another case, the patient sustained an injury 3 weeks after prosthesis implantation that caused an open fracture and led to chronic osteitis (Figure 2). In a third case, prosthesis removal prior to referral to our hospital led to complicated fractures of the femur and tibia (Figure 3).
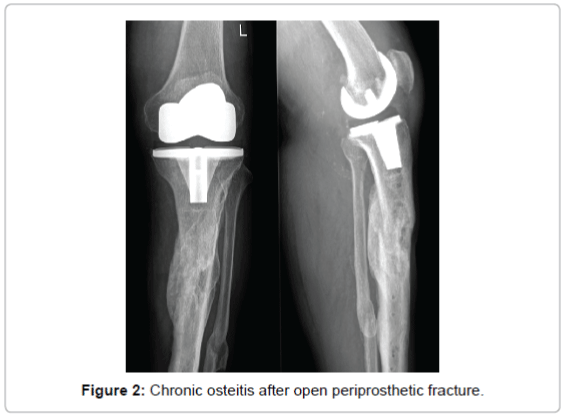
Figure 2: Chronic osteitis after open periprosthetic fracture.
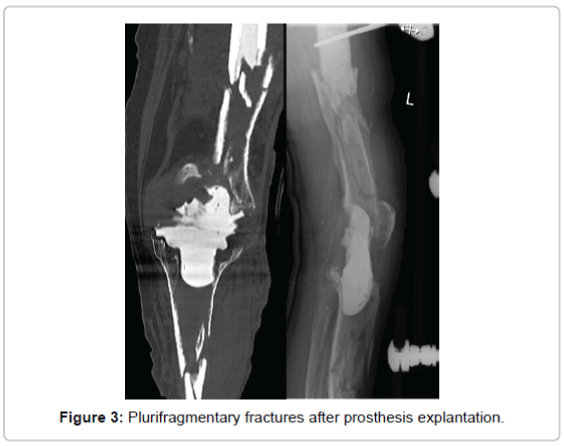
Figure 3: Plurifragmentary fractures after prosthesis explantation.
Soft tissue defects
Two patients had wound healing deficiencies prior to amputation, and 2 other patients developed a large tissue defect at the site of the prosthesis (Figure 4).
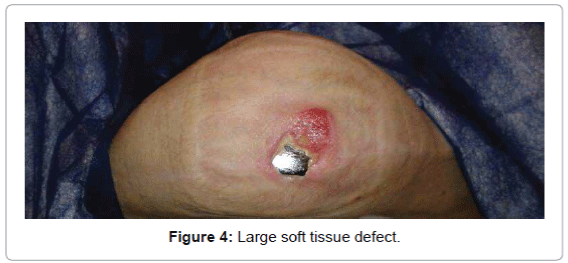
Figure 4: Large soft tissue defect.
Iatrogenic complications
Three complications were iatrogenic and developed prior to referral to our hospital.
As mentioned above, removal of the prosthesis led to complicated fractures of the femur and tibia in one patient (Figure 3).
One patient with a large tissue defect was treated with a wound healing cream by his general practitioner for two weeks prior to referral to an orthopedic surgeon (Figure 4).
Finally, one patient had a history of self-mutilation prior to knee prosthesis implantation and continued self-mutilating her operated knee with needles after total knee arthroplasty.
Limitations
As this study had a retrospective design, it was purely observational. The study sample was low because above knee amputation is a rare complication following total knee arthroplasty. Nonetheless, we were able to include all eligible patients seen at our hospital during the past ten years in this study. As we are a center specializing in the field of periprosthetic infections, we have a bias toward severe infectious cases that are referred to our institution by smaller hospitals.
Discussion
The principal result of this study is that the prosthesis-related indications for above knee amputation after total knee arthroplasty are always multi-factorial; an infection is always present in addition to at least two other factors, even in the case of a major event, such as necrotizing fasciitis, an accident causing an open fracture or a large soft tissue defect.
Total knee arthroplasty is a very successful operation. However, a constantly aging population leads to an increasing number of implantations of these prostheses [5]. Consequently, exchange operations and the lifetime risk for severe complications, such as periprosthetic infections, will also increase. As a center specialized in the treatment of infected joint endoprostheses, we receive many referrals with severe infections from other hospitals (13 out of 16 of the presented cases), where complete eradication of the infection can only be achieved by removal of all components and through arthrodesis or above knee amputation [14,15]. Many studies support the fact that an arthrodesis provides a better functional outcome compared to a transfemoral amputation and should therefore be considered the treatment of choice in cases of persistent infection after failed two-stage revision surgery for infected total knee arthroplasty [15,35]. However in cases with severe bone loss and extensive soft tissue damage following repeatedly failed two-stage revision surgeries, the possibility of a knee arthrodesis may be ruled out [35], leaving a transfemoral amputation as the only option to definitively resolve the infection according to Fedorka et al. [31]. The present study supports this fact as the average time from primary implantation to amputation being 95.7 months (7.9 years) and the average number of operations prior to above knee amputation being 7.8 are comparable results to those of Fedorka et al., who showed an average time from primary implantation to amputation of 6 years and an average number of 5 procedures prior to amputation [30]. Presumably, with every revision surgery the bone stock decreases and the soft tissue coverage is at risk of compromising the option of a knee arthrodesis.
In only two of our patients, a transfemoral amputation was the primary procedure of choice to treat the periprosthetic infection. Both patients had an infection caused by multiple bacteria, both had a large tissue defect, one had sepsis, whilst the other had a soft tissue abscess. Large soft tissue defects and a rapidly progressive infection excluded the possibility of other treatment options, leaving an above knee amputation as the only possible salvage procedure in order to control the infection.
Avoidable complications in the present study were those that were iatrogenic. Some of these complications can be avoided, if the treatment of infected knee prosthesis is led by an orthopedic surgeon with particular experience in this field.
Knee prosthesis explantation can cause fractures of adjacent bones; however, in one case reported here, the explantation caused devastating plurifragmentary fractures of the femur and tibia. Therefore, whenever possible, we suggest that explantations should be performed by experienced orthopedic surgeons to minimize this risk.
Patients with large tissue defects should immediately be referred to an orthopedic surgeon who then treats the patient in consultation with a plastic surgeon. In one case, amputation could have been avoided if the patient had been referred to our institution sooner. That patient’s condition could not be adequately treated by a general practitioner.
Knee prosthesis implantation must always be carefully planned. In our series, one patient had a history of self-mutilation that was not resolved prior to the knee prosthesis implantation. In this case, continuous self-inflicted injuries led to infection and subsequent above knee amputation after total knee arthroplasty. Careful selection of patients for knee prosthesis implantation may have avoided this outcome.
In conclusion, the decision to perform an above knee amputation after total knee arthroplasty is made on an individual basis for each patient separately. It can be based on the presence of an infection with systemic relevance (e.g., sepsis), in which case an amputation is a life-saving procedure, or the presence of an infection with local bone stock loss of the affected limb (e.g., osteitis or fracture), for which limb salvage is not expected.
Author Contributions
Philip J.F. Leute and Hans-Michael Klinger both wrote the ethics proposal and wrote the manuscript. Philip J.F. Leute and Ahmed Hammad gathered the data and computed the statistics. Frank Braatz revised and wrote the manuscript and performed some of the operations.
The authors declare that they have no conflict of interest.
