Commentary - (2017) Volume 6, Issue 5
Brown tumors are focal bone lesions, caused by increased osteoclastic activity and fibroblastic proliferation, encountered in patients with uncontrolled hyperparathyroidism (HPT). They can be located in any part of the skeleton, but are most frequently encountered in the ribs, clavicles, extremities, and pelvic girdle. Clinically significant lesions in the craniofacial bones are rare Brown tumors are focal reactive osteolytic lesions caused by hyperparathyroidism (HPT) and represent the terminal stage of the hyperparathyroidism-dependent bone pathology. Nowadays, the manifestation of hyperparathyroidism with these lesions is extremely rare in developed countries, because of the early detection of the disease, using routine laboratory examination and early treatment of that.
These benign lesions present similar radiologic findings as bone metastasis, which makes the diagnosis difficult Brown tumors are focal bone lesions, caused by increased osteoclastic activity and fibroblastic proliferation, encountered in patients with uncontrolled hyperparathyroidism (HPT). They can be located in any part of the skeleton, but are most frequently encountered in the ribs, clavicles, extremities, and pelvic girdle. Clinically significant lesions in the craniofacial bones are rare Brown tumors are focal reactive osteolytic lesions caused by hyperparathyroidism (HTP) and represent the terminal stage of the hyperparathyroidism-dependent bone pathology.
Nowadays, the manifestation of hyperparathyroidism with these lesions is extremely rare in developed countries, because of the early detection of the disease, using routine laboratory examination and early treatment of that. These benign lesions present similar radiologic findings as bone metastasis, which makes the diagnosis difficult.
Keywords: Bones; Musculoskeletal; Neoplasia; Brown; MR; CT; PET
1. To demonstrate the Multi-Modality Imaging features of Brown tumors of Primary Hyperparathyroidism.
2. To highlight spectrum of associated skeletal manifestations in Primary Hyperparathyroidism.
Brown tumors are focal bone lesions, caused by increased osteoclastic activity and fibroblastic proliferation, encountered in patients with uncontrolled hyperparathyroidism (HPT) [1-3].
They can be located in any part of the skeleton, but are most frequently encountered in the ribs, clavicles, extremities, and pelvic girdle Figures 1-3.
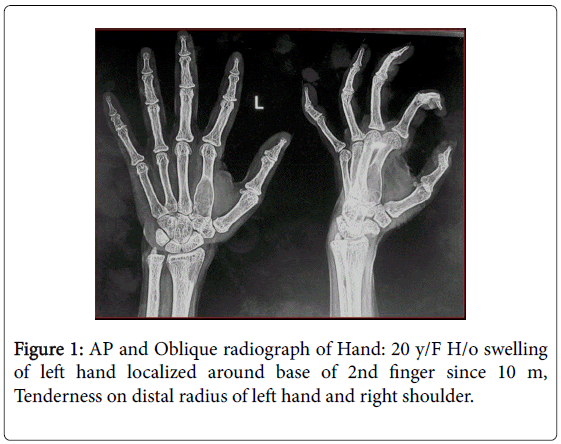
Figure 1: AP and Oblique radiograph of Hand: 20 y/F H/o swelling of left hand localized around base of 2nd finger since 10 m, Tenderness on distal radius of left hand and right shoulder.
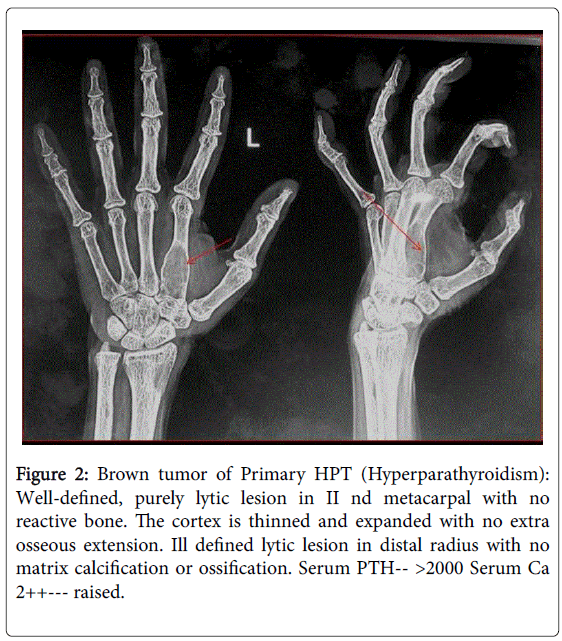
Figure 2: Brown tumor of Primary HPT (Hyperparathyroidism): Well-defined, purely lytic lesion in II nd metacarpal with no reactive bone. The cortex is thinned and expanded with no extra osseous extension. Ill defined lytic lesion in distal radius with no matrix calcification or ossification. Serum PTH-- >2000 Serum Ca 2++--- raised.
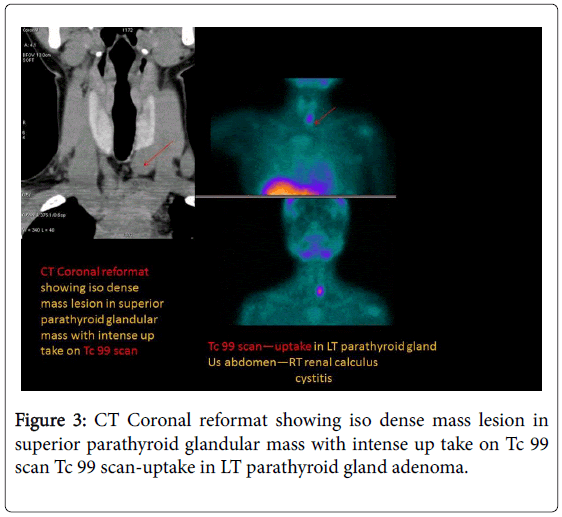
Figure 3: CT Coronal reformat showing iso dense mass lesion in superior parathyroid glandular mass with intense up take on Tc 99 scan Tc 99 scan-uptake in LT parathyroid gland adenoma.
Clinically significant lesions in the craniofacial bones are rare Brown tumors are focal reactive osteolytic lesions caused by hyperparathyroidism (HPT) and represent the terminal stage of the hyperparathyroidism-dependent bone pathology. Nowadays, the manifestation of hyperparathyroidism [4,5] with these lesions is extremely rare in developed countries, because of the early detection of the disease, using routine laboratory examination and early treatment of that.
These benign lesions present similar radiologic findings as bone metastasis, which makes the diagnosis difficult Brown tumors are focal bone lesions in Figure 4, caused by increased osteoclastic activity and fibroblastic proliferation [6], encountered in patients with uncontrolled hyperparathyroidism (HPT).
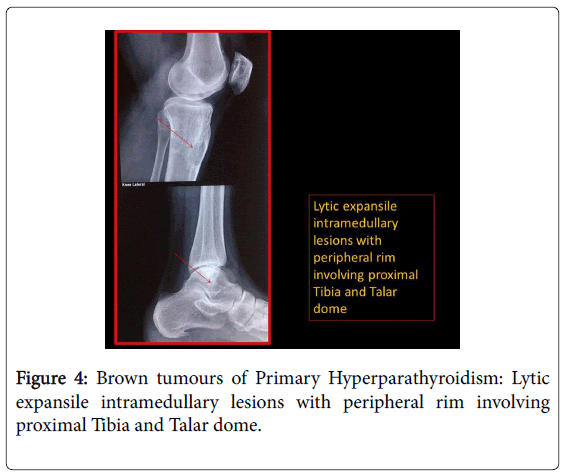
Figure 4: Brown tumours of Primary Hyperparathyroidism: Lytic expansile intramedullary lesions with peripheral rim involving proximal Tibia and Talar dome.
They can be located in any part of the skeleton, but are most frequently encountered in the ribs, clavicles, extremities, and pelvic girdle. Clinically significant lesions in the craniofacial bones [7] are rare Brown tumors are focal reactive osteolytic lesions caused by hyperparathyroidism (HTP) and represent the terminal stage of the hyperparathyroidism-dependent bone pathology. Nowadays, the manifestation of hyperparathyroidism with these lesions is extremely rare in developed countries, because of the early detection Figure 5 of the disease, using routine laboratory examination and early treatment of that. These benign lesions present similar radiologic findings as bone metastasis, which makes the diagnosis difficult.
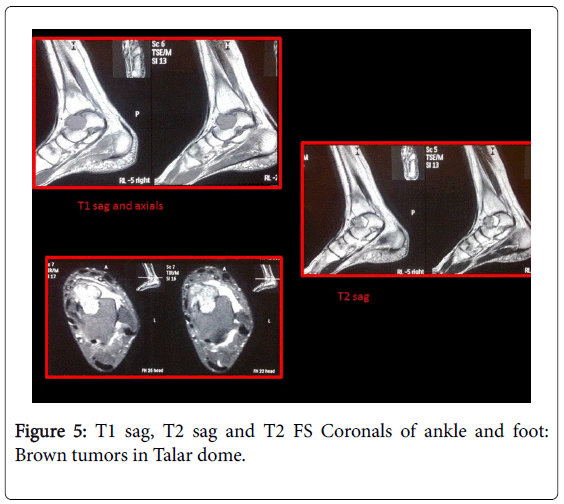
Figure 5: T1 sag, T2 sag and T2 FS Coronals of ankle and foot: Brown tumors in Talar dome.
A solitary brown tumor might be confused with solitary bone cyst, aneurismal bone cyst, and giant cell tumor or giant cell [8] reparative granuloma. With multiple brown tumors, differential diagnosis includes: osteolytic metastasis, multiple myeloma, multiple bone cysts, etc. It is the presence of sclerotic margin that excludes metastasis.
The Radio-Pathology correlates of Brown Tumors are described with differential diagnosis. Plain Radiography, CT, MRI features of Brown tumors and associated findings in Primary HPT are elucidated. Brown tumor [9] (also known as osteitis fibrosa cystica or rarely osteoclastoma) is one of the manifestations of hyperparathyroidism in Figure 6. It represents a reparative cellular process, rather than a neoplastic process. Brown tumor (also known as osteitis fibrosa cystica or rarely osteoclastoma) is one of the manifestations of hyperparathyroidism [10]. It represents a reparative cellular process, rather than a neoplastic process. Brown tumors have a slightly greater frequency in primary than in secondary hyperparathyroidism (3% versus 2%). However, secondary hyperparathyroidism is much more common than primary hyperparathyroidism; therefore most of brown tumors that are seen are associated with secondary hyperparathyroidism.
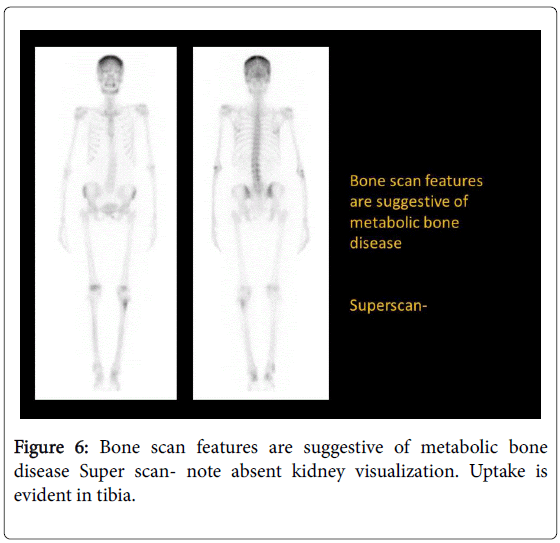
Figure 6: Bone scan features are suggestive of metabolic bone disease Super scan- note absent kidney visualization. Uptake is evident in tibia.
In chronic renal disease, continual and excessive urinary calcium excretion can lower serum calcium level and lead to a rise in parathyroid hormone secretion. This results in mobilization of skeletal calcium through rapid osteoclastic turnover of bone to maintain normal serum calcium levels [11]. In localized regions where bone loss is particularly rapid, hemorrhage, and reparative granulation tissue, with active, vascular, proliferating fibrous tissue may replace the normal marrow contents, resulting in a brown tumor. Hemosiderin imparts the brown color (hence the name of the lesion).
Plain radiograph
Well-defined, purely lytic lesions that provoke little reactive bone. The cortex may be thinned and expanded, but will not be penetrated.
CT
Attenuation values on CT will be in the range of blood and fibrous tissue.
MRI
The MRI appearance depends on the relative proportion of its components. The lesions therefore may be solid, cystic, or mixed. Solid components are intermediate to low intensity on T1- and T2-weighted images, while the cystic components are hyper intense on T2-weighted images and may have fluid-fluid levels [12,13]. T1 C+ (Gd): there can be enhancement of the solid component and septa.
Angiography
Lesions are usually hyper vascular.
Nuclear medicine
Bone scan often shows intense uptake Figures 7 and 8.
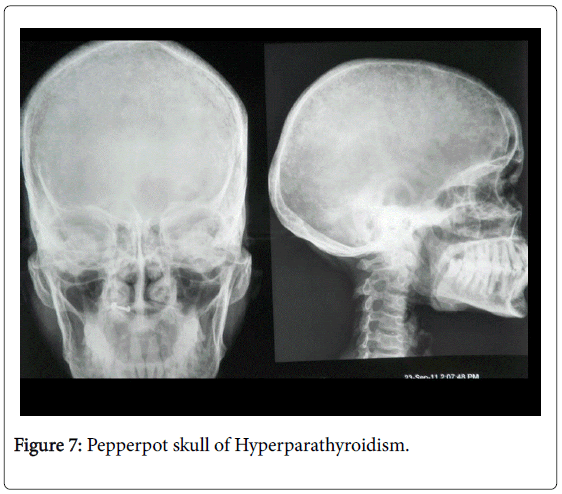
Figure 7: Pepperpot skull of Hyperparathyroidism.
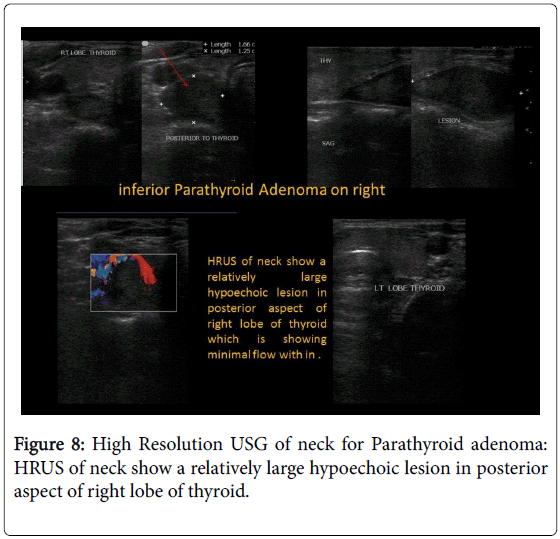
Figure 8: High Resolution USG of neck for Parathyroid adenoma: HRUS of neck show a relatively large hypoechoic lesion in posterior aspect of right lobe of thyroid.
This exhibit serves as a resource for Imaging of Brown tumors what a resident must know.
