Case Report - (2016) Volume 5, Issue 1
Objective: We report a rare case of revision total knee arthroplasty for monoarthritis of the knee due to rheumatoid arthritis (RA). Case: The patient was a 72-year-old woman, who underwent revision surgery at 8 years and 7 months after left unicompartmental knee arthroplasty. Bacteriological examination of the synovial fluid was negative, and no crystals were found by microscopic examination. When the Knee Society score was determined, the knee score was 43 points and the function score was 45 points. No periprosthetic radiolucent lines were observed and there was no loosening. Erosion of the lateral femoral and tibial condyles was observed. CRP 3.6 mg/dL, erythrocyte sedimentation rate 129 mm/h, RF 101 U/mL, MMP3 732.2 ng/mL, anti-CCP antibody 190.3 U/mL. Revision TKA was done with a NexGen CR Flex (Zimmer Corp.) RA was diagnosed by histopathological examination of the synovium. Detailed investigation with bone scintigraphy and gallium scintigraphy did not identify inflammation of any other joints. However, pain and swelling of the right knee joint appeared 5 months after revision surgery, and right TKA was performed. Histopathological examination of the synovium resected from the right knee also revealed findings typical of RA. Discussion: Revision TKA is likely to increase in the future because of more patients undergoing UKA and an increase in the age of onset of RA. If knee pain occurs in patients after unicompartmental knee arthroplasty, monoarthritis due to RA should be considered as a possibility. Accordingly, we should follow patients after UKA while keeping the possibility of RA in mind.
Keywords: Monoarthritis; Revision; Rheumatoid arthritis; Total knee arthroplasty; Unicompartmental arthroplasty
Unicompartmental knee arthroplasty (UKA) is less invasive than total knee arthroplasty (TKA), and is performed in many patients including elderly and non-obese persons. It has been reported that the indications for UKA are an intact anterior cruciate ligament (ACL), intact contralateral cartilages, and absence of inflammatory diseases such as rheumatoid arthritis (RA) [1].
We report a case of revision TKA after UKA following the onset of left knee arthritis caused by RA at approximately 8 years after the initial operation.
The patient was a 72-year-old woman whose chief complaint was left knee pain. She has a past history of asthma, but no history of arthritis. In January 2006 (at 64 years old), she had undergone left medial UKA (Oxford®, Biomet, Warsaw, IN, USA) at another hospital. At that time, rheumatoid factor (RF) was negative and the outcome of surgery was satisfactory. She subsequently presented to the previous hospital with left knee pain of spontaneous onset at 7 years and 9 months after UKA. After 8 months of conservative treatment at that hospital, she was referred to our department for surgery due to exacerbation of left knee pain and swelling. She had no symptoms such as morning stiffness of the hands.
Findings at the first visit
Examination of the left knee joint: The joint was tender and swollen. The range of motion (ROM) was 0 degrees of extension and 130 degrees of flexion, with a floating patellar. The aspirated synovial fluid (20 mL) was yellow and slightly cloudy. Bacteriological examination of the synovial fluid was negative, and no crystals were found by microscopic examination. When the Knee Society Score was determined, the knee score was 43 points and the function score was 45 points.
Systemic findings: There was no tenderness or swelling of other joints.
Findings on plain X-ray films of the left knee: No periprosthetic (Figure 1) radiolucent lines were observed and there was no loosening. Erosion of the lateral femoral and tibial condyles was observed.
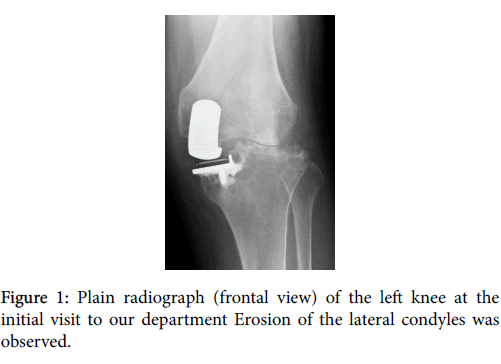
Figure 1: Plain radiograph (frontal view) of the left knee at the initial visit to our department Erosion of the lateral condyles was observed.
Laboratory test results: white blood cell (WBC) 6700/μL, uric acid 3.8 mg/dL, hemoglobin (Hb) A1c 6.2%, c-reactive protein (CRP) 3.6 mg/dL, erythrocyte sedimentation rate (ESR)129 mm/h, RF 101 U/mL, immunoglobulin G (IgG) 2451 mg/dL, matrix metalloproteinase-3 (MMP-3) 732.2 ng/mL, anti-cyclic citrullined peptide(CCP) antibody 190.3U/mL, creatine phosphokinase (CPK) 153 u/L, alkaline phosphatase (ALP) 308 U/L, Ca 8.6 mg/dL, P 3.3 mg/dL, cancer antigen (CA)-125 13.2 U/mL, CA19-9 4.2 U/mL, carcinoembryoric antigen (CEA) 1.9 ng/mL, superconducting conductor (SCC) 0.7 mg/mL, bone-specific ALP 11.5 μg/L, these based on these laboratory data obtained at the initial examination, RA was suspected. However, the patient had monoarthritis, and her score according to the 2010 American College of Rheumatology (ACR)/European League Against Rheumatism (EULAR) classification criteria for RA was only 5 points, so a definite diagnosis of RA was not made.
Operative findings
The patient underwent revision TKA at 10 months after the onset of left knee arthritis (8 years and 7 months after UKA). There was marked outgrowth of the synovium in the left knee joint, and erosion of the lateral condyles of the femur and tibia (Figure 2a). The ACL was intact, and backward gliding of the polyethylene insert was observed with no loosening of the components. The posterior cruciate ligament (PCL) was also intact. A defect 25 mm in depth was observed in the proximal medial surface of the tibia (Figure 2b). Revision TKA was done with a NexGen® PCL-retaining (CR) Flex (Zimmer, Warsaw, IN, USA). The tibial component was cemented with 10 mm medial and 5 mm lateral augmentation using a stem extension that was 12 mm in diameter and 100 mm in length. A 12 mm thick polyethylene insert was used, and the patella was not replaced (Figure 3).
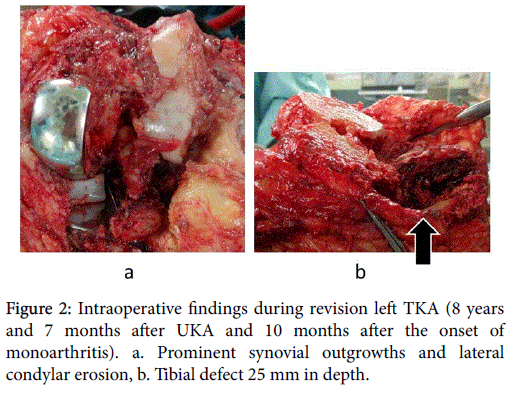
Figure 2: Intraoperative findings during revision left TKA (8 years and 7 months after UKA and 10 months after the onset of monoarthritis). a. Prominent synovial outgrowths and lateral condylar erosion, b. Tibial defect 25 mm in depth.
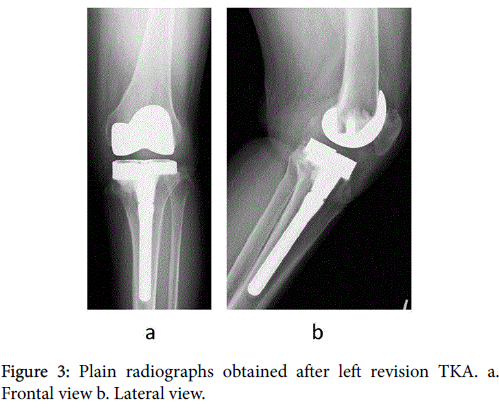
Figure 3: Plain radiographs obtained after left revision TKA. a. Frontal view b. Lateral view.
Histopathological examination of the synovium
The synovial tissue resected at revision surgery showed papillary growth with infiltration of lymphocytes and plasma cells, as well as fibrin clot formation, which were findings that suggested active RA (Figure 4).
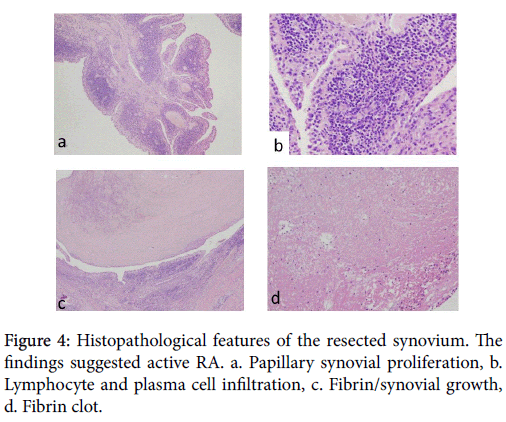
Figure 4: Histopathological features of the resected synovium. The findings suggested active RA. a. Papillary synovial proliferation, b. Lymphocyte and plasma cell infiltration, c. Fibrin/synovial growth, d. Fibrin clot.
Postoperative course
Bone scintigraphy (Figure 5a) and gallium scintigraphy (Figure 5b) did not identify any inflammation elsewhere in the body.
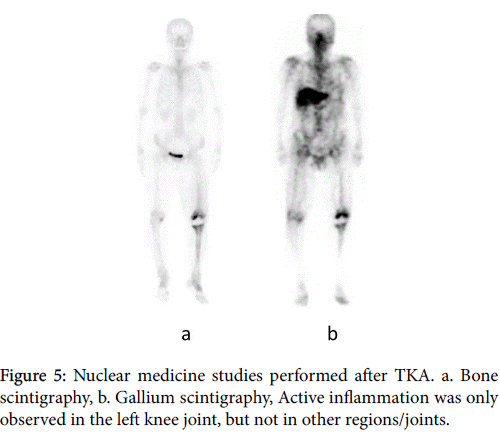
Figure 5: Nuclear medicine studies performed after TKA. a. Bone scintigraphy, b. Gallium scintigraphy, Active inflammation was only observed in the left knee joint, but not in other regions/joints.
Pain in the left knee joint resolved after revision TKA and the patient was made good progress. Medical therapy for RA was considered, but disease modified anti-rheumatic drugs (DMARDs) such as methotrexate were not prescribed because the patient had a high Krebs von den Lungen-6 (KL-6) level (981 U/mL) and there was no arthritis of other joints.
However, pain and swelling of the right knee joint appeared 5 months after revision surgery (9 years after UKA), so oral administration of salazosulfapyridine was started. Her right knee pain persisted, and right TKA was performed 7 months after revision surgery. Histopathological examination of the synovium resected from the right knee also revealed findings typical of RA. After the onset of right knee arthritis, the patient satisfied the 2010 ACR/EULAR classification criteria for RA. On examination at 13 months after revision TKA of the left knee (6 months after right TKA), she had no knee joint pain. The ROM was 0 degrees of extension/120 degrees of flexion for the left knee and 0 degrees of extension/100 degrees of flexion for the right knee. Assessment of the Knee Society score showed that the knee score was 91 points and the function score was 75 points. Arthritis was not observed in other joints and the outcome was satisfactory.
With regard to the results of TKA and UKA, a 27-year registry study of 4,713 patients in Finland showed that the 10-year survival rate of the prosthesis was 93.3% after TKA versus 80.6% after UKA, indicating that the outcome was inferior for UKA compared with TKA [2]. However, it has been reported that better results can be obtained with UKA if the surgical indications are followed carefully. Barrett et al. described the importance of observing the indications for UKA [3], while Katsuragawa et al. reported that excluding active arthritis before surgery is required for successful UKA [4]. In addition, Berend et al. reported that the failure rate of UKA increases when the body mass index (BMI) of the patient exceeds 32 kg/m [2,5].
Katsuragawa et al. found that UKA was unsatisfactory in 13% of patients 3). Among the reasons for inferior results, aseptic loosening is reported to be the most frequent, while progression of arthritis in other compartments (lateral or patellofemoral joint) is also a problem [6-12]. Other causes that have been reported include instability, infection, arthrofibrosis, persistent pain, polyethylene wear, and fracture, but there have been no reports of RA leading to revision surgery [6-12].
Occurrence of RA is rare after UKA. Tada et al. reported the onset of RA in 1 out of 382 knees after off-label UKA [13]. In addition, Goto et al. reported RA in 2 patients (2 knees) out of 109 patients (115 knees) at 3 years and 1 year after surgery, respectively, with both patients being followed up [14]. In our patient, UKA was performed initially because RA was excluded by a negative RF test and the absence of other joints with arthritis. Since left knee function was good for nearly 8 years after UKA and arthritis affecting other joints was not observed for 9 years, we concluded that revision TKA was performed for RA monoarthritis in our patient.
Monoarthritis is not usually caused by RA and its diagnosis is difficult. Binard et al. reported that RA was not diagnosed in patients with early monoarthritis and no previous history of arthritis [15]. In contrast, Jeong et al. reported that RA was eventually diagnosed in 18.1% of patients who had monoarthritis, with detection of anti-CCP antibody, RF and bone erosions being useful for making the diagnosis [16]. Tanaka et al. found progression to RA after 6 months or longer in 14% of patients with knee joint edema, and stated that elevation of interleukin (IL)-1β and IgG-RF in synovial fluid was useful for diagnosis [17]. In our patient, histopathological findings indicated that monoarthritis of the knee was due to RA not satisfying the ACR/ EULAR classification criteria. She had monoarthritis of the left knee with no prior history of arthritis, but her monoarthritis progressed to RA satisfying the 2010 ACR/EULAR classification criteria after arthritis also affected the right knee. This outcome was different from the findings of Binard et al. [15].
In our patient, adequate treatment for RA was not provided because of delay in making the diagnosis, the high KL-6 level, and no arthritis affecting other joints. If she had received effective treatment for RA after the onset of monoarthritis, revision TKA or RA of the right knee might have been prevented. Revision TKA is likely to increase in the future because of more patients undergoing UKA and an increase in the age of onset of RA. Therefore, early treatment should be provided in similar cases.
TKA is recommended for revision surgery after UKA [18]. Saragaglia et al. [19] reported that TKA was conducted for revision surgery in 87% of 426 joints, (posterior stabilized(PS) type in 62.7%, CR type in 33.2%, and rotating hinge in 4.1%), while ipsilateral UKA was done in 7.7%, and they recommended TKA due to difficulty in using a similar implant for revision [19]. Our patient had a lateral bone defect with intact PCL, so revision surgery was performed with CR type TKA using augmentation and stem extension.
We reported a rare case of revision TKA for monoarthritis of the knee due to RA after UKA. If knee pain occurs after UKA, RA monoarthritis should be considered because this surgery is being performed at a younger age, the number of operations is increasing, and onset of RA at an advanced age is being recognized in some cases. If RA occurs after UKA, early treatment is necessary to prolong the survival of the implant and prevent inflammation of other joints. Accordingly, we should follow patients after UKA while keeping the possibility of RA in mind.
None
