Research Article - (2015) Volume 4, Issue 3
Objective: To verify the effectiveness of custom-molded FO (Foot Orthoses) on kinetic parameters, pain, and disability in RA patients. Methods: Patients with RA were randomized into FO and no orthoses groups. Kinetic parameters were assessed using a foot pressure system, foot pain was evaluated using the pain subscale of the American Orthopaedic Foot and Ankle Society (AOFAS) ankle-hindfoot scale, and disability was evaluated by the total score of the AOFAS anklehindfoot scale and by the Health Assessment Questionnaire for RA. Results: Analyses were performed on data collected at baseline and after 2 months of intervention. Thirty-three women (mean age, 53.0 ± 10.97 years; mean disease duration, 12.2 ± 7.54 years) were evaluated. No differences in the kinetic parameters, and small, but non-significant, improvements in the pain and disability measures were observed in the FO group. Conclusions: FO without other conservative treatments did not have a significant effect on the pain and disability in RA patients. Additional, larger trials are needed to investigate the effects of these devices combined with physical therapy in similar patients. Trial registration: http://www.ensaiosclinicos.gov.br/rg/RBR-24ydf6/, RBR-24ydf6.
Keywords: Rheumatoid arthritis; Foot orthoses; Clinical trial; Disability; Pain; Foot plantar pressure; Foot care
Rheumatoid arthritis (RA) is a chronic inflammatory disease with a reported prevalence of 0.3-1.0% [1]. Foot impairment occurs in 85– 100% of all RA patients [2], with erosive synovitis being the primary cause for the high levels of pain and/or disability in these patients [3].
The first clinical signs on the feet generally appear in the first three years of the disease [4]. Stiffness and pain in the metatarsophalangeal joints, increase in plantar pressure on the forefoot, collapse of the longitudinal arch, and rear foot/ankle dysfunction are the most common symptoms of RA in the feet [5].
Conservative treatment methods, including foot orthoses (FO), are often used in RA patients to reduce pain, prevent and control joint damage, and improve function [6]. Despite previous studies having demonstrated some specific improvements in the level of pain, the use of FO has yielded inconsistent results in terms of important outcomes such as disability [7]. These inconclusive results can be attributed to the lack of standardized intervention programs used in the previous studies. There is currently no consensus concerning the most appropriate type (custom-molded or unshaped), materials, and duration of wearing of the FO, as well as whether combined use with therapeutic footwear is needed or not, and this may have lead to an overestimation of the results [3,7].
With this in mind, the aim of the present study was to assess the effects of FO on kinetic parameters, pain, and disability in patients with RA.
Study design and sample size calculation
We conducted a randomized clinical trial study according the CONSORT criteria. Sample size calculation indicated that 32 subjects were needed to detect a difference of 20 points in the AOFAS scale, with a standard deviation of 19 points, a significance level of 5%, and 80% power, based on the prevalence of rheumatoid arthritis of the population of Salvador, Brazil (0.5%).
Patients
Patients were enrolled from the Arthritis Rheumatoid Service of the Bahia School of Medicine and Public Health from October 2013 to February 2014.
Patients were eligible for inclusion if they were between 18 and 75 years of age; had a diagnosis of RA by a rheumatologist satisfying the American Rheumatism Association revised criteria for RA, with active RA defined by a Disease Activity Score in 28 joints ≥ 2.7 [8]; foot pain and demonstrated ability of walking with or without assistive devices. Patients were excluded if they had neurologic dysfunction, cognitive deficits on the Mini Mental State Examination [9], skin lesions, surgery in the lower limb, or were pregnant.
The study was approved by the Research Ethics Committee of the Estacio of Bahia University Center (no. 657.528) and BAHIANA School of Medicine and Public Health (no. 746.121). The eligible subjects received an explanation of the aims and methods of this study and all agreed to sign an informed consent form. The trial is registered at http://www.ensaiosclinicos.gov.br/rg/RBR-24ydf6/ and the registration number is RBR-24ydf6.
Interventions
The intervention (FO) group received FO, and the control group received no orthoses. Randomization was based on a randomization roll die and was conducted by one of the research members after the first assessment to ensure a blind pretest. At the first visit, a subtalar neutral joint cast was designed for all patients, regardless of group allocation.
The functional FO consisted of a medial longitudinal arch support, medial and lateral heel posts to improve heel stabilization and reduce excessive eversion/inversion, and a metatarsal pad to support the transverse arch and reduce forefoot pressure. To ensure the best fit for many types of women’s footwear and avoid treatment discontinuation [10], the FO were custom-molded to ¾ length of the insole, and fabricated with thermoformable polyurethane base with a 4-mm thickness plastazote coverage. All subjects were instructed to not modify their treatment program, and the subjects in the FO group were instructed to use the insoles for at least 4 hours a day and how to care for their insoles.
Clinical assessments
The variables were evaluated at baseline and 2 months after starting the intervention. Basic sociodemographic and clinical data were recorded on baseline.
Kinetic variables measurement
Load distribution on the feet and left and right center of gravity oscillation were recorded in bipedal barefoot support using a Footwork® foot pressure system. This system uses a force plate with 4-mm thickness and 2704 calibrated capacitive sensors with an analog conversion rate of 16 bits and frequency of 150 Hz, and generates data to be analyzed by the Footwork® software, version 2.9.8.0 ([AM3 – Berkshire –UK). These data were obtained from an average of 3 samples, 20 s each.
Pain and disability measurements
The pain subscale of the American Orthopaedic Foot and Ankle Society (AOFAS) ankle-hindfoot scale was used to assess foot pain. This subscale consists on 4 items measuring the level of foot pain as none (40 points); mild, occasional (30 points); moderate, daily (20 points); and severe, almost always present (zero points). The AOFAS scale is an internationally validated and tested scale, which has been translated into Portuguese [11], and is considered the most recommended scale for functional assessment of the foot-ankle complex in Brazil [12]. This instrument consists of 9 items separated into 3 categories: pain (40 points), functional aspects (50 points), and alignment (10 points). The total score is 100 points, which indicates a normal degree of functionality. Disability was evaluated by the total score of the AOFAS scale and by the Stanford Health Assessment Questionnaire (HAQ). The HAQ is the most frequently used validated questionnaire in clinical trials to assess disability in people with RA [13]. This instrument is divided in 8 sections: dressing, arising, eating, walking, reaching, gripping, and activities. For each section, the level of disability is scored from 0 (without any difficulty) to 3 (unable to perform). The final score is the average of the scores for all 8 sections.
Statistical analysis
We used descriptive statistics for analysis of sociodemographic and clinical data. Data of continuous variables were analyzed with measures of central tendency and dispersion, and expressed as the mean and standard deviation. Categorical or dichotomous variables were analyzed with measures of frequency and expressed as percentages. We performed statistical tests (Shapiro-Wilk and Kolmogorov-Smirnov) to evaluate the normality and homogeneity of variance for all variables. Student’s t test was used to compare the mean intra- and inter-group differences of the variables. The differences between average values were expressed with a confidence interval of 95%. We used the chisquare test to compare proportions. All survey data were analyzed using SPSS version 17.0 (SPSS Inc., Chicago, IL).
Out of the identified 113 patients, 59 patients met the eligibility criteria and were randomized to the FO (n=30) and no orthoses groups (n=29). Figure 1 summarizes the patients and enrollment process. A total of 33 female patients (18 and 15 in the FO group and no orthoses groups, respectively) completed the study and were assessed for the outcomes.
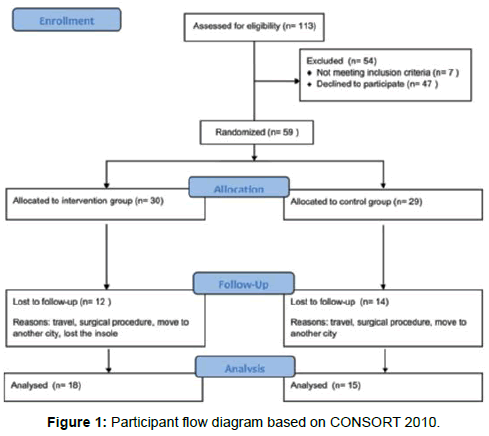
Figure 1: Participant flow diagram based on CONSORT 2010.
Table 1 shows the baseline demographic and clinical characteristics of the patients in each group. At baseline, no significant differences were found between the groups. Of the included 33 women (mean age, 53.0 ± 10.97 years; mean disease duration, 12.2 ± 7.54 years; active disease level, ≥3.3), 18 patients (54.5%) had a previous diagnosis of hypertension, 3 patients (9%; 2 in the FO group) reported smoking, and 5 (15%; 2 in the FO group) reported consuming alcoholic beverage on weekends. The kinetic parameters (assessed on bipedal barefoot support), pain, and disability status were similar, with no statistically significant differences observed between the groups.
| Foot Orthoses Group N=18 | Control Group N=15 | |
|---|---|---|
| Demographics Age (years)* | 54.7 ± 11.3 | 51.0 ± 10.6 |
| Economic class (A1:B1:B2:C1:C2) | 1:0:5:4:8 | 0:1:4:6:4 |
| Ethnicity (Caucasian:African:Mulatto) | 3:7:8 | 1:8:6 |
| Dominant leg (right:left) | 14:4 | 14:1 |
| BMI (kg/m2)* | 25.7 ± 5.5 | 27.7 ± 5.8 |
| Educational level (illiterate:highschool:college) | 3:13:2 | 3:9:2 |
| Clinical | ||
| Disease duration (years)* | 11 ± 6.5 | 10 ± 8.9 |
| DAL (active:remitting)2 | 18:0 | 15:0 |
| Anti-inflammatory drugs | 18 | 15 |
| Foot deformities and pain | 18 | 15 |
| Level ofphysical activity (sedentary:sporadicpractitioner) | 16:2 | 12:3 |
| Kinetic parameters* Rearfoot:forefoot load (%) | 53.0 ± 6.4: 47.0 ± 6.4 | 53.8 ± 5.9: 46.2 ± 5.9 |
| Right:left foot load (%) | 53.5 ± 4.9: 46.5 ± 4.7 | 53.6 ± 5.1: 46.4 ± 5.1 |
| Foot GC oscillation- FP (right:left) (cm2) | 0.5 ± 0.4: 0.5 ± 0.4 | 0.7± 1.0: 0.5 ± 0.3 |
| Foot GC oscillation – SG (right:left) (cm2) | 2.2 ± 1.3: 2.5 ± 1.1 | 1.9 ± 0.5: 2.1 ± 0.8 |
| Disability (AOFAS)* | ||
| Pain | 10.6 ± 11.1 | 12.0 ± 12.6 |
| Function | 32.2 ± 9.3 | 34.0 ± 6.5 |
| Alignment | 1.4 ± 2.3 | 1.0 ± 2.8 |
| Total | 43.3 ±19.7 | 47.0 ± 19.5 |
| Disability (HAQ)* | 1.7 ± 0.7 | 1.5 ± 0.6 |
Economic class: A1, B1 (high economic level); B2, C1, and C2 (moderate economic level) based on the Brazilian Research Enterprises Association definition. Abbreviations: AOFAS, American Orthopaedic Foot and Ankle Society ankle-hindfoot scale; DAL, disease activity level; FP, frontal plane; GC, gravity center; BMI, body mass index; SG, sagittal plane; HAQ, Health Assessment Questionnaire. * Values are presented as mean ± standard deviation
Table 1: Baseline characteristics of the two groups.
After 2 months of FO intervention, no significant intra- and intergroup differences could be found in the pain and disability. However, there was a small, albeit non-significant, decrease in the pain and foot and ankle disability (American Orthopaedic Foot and Ankle Society [AOFAS] score) in the FO group, and a small increase in the control group. The kinetic parameters did not show any intra- and inter-group differences. Table 2 displays the results after 2 months of treatment as compared to baseline for both groups.
| Foot Orthoses Group | Control Group | |||||
|---|---|---|---|---|---|---|
| Before intervention | After intervention | p* | Before intervention | After intervention p* | ||
| Kinetic parameters | ||||||
| Rearfoot: forefoot load | 53.1 ± 6.5: 47 ± 6.4 | 53.6 ± 6.5: 46.3 ± 6.5 | 0.433: 0.339 | 53.9 ± 5.9: 46 ± 5.9 | 54.4 ± 5.9: 45.7 ± 5.9 | 0.636 0.635 |
| Right: left foot load | 53.5 ± 4.9: 47 ± 5.3 | 52.1 ± 5.9: 48.5 ± 6.1 | 0.086: 0.086 | 53.6 ± 5.1: 46.4 ± 5.1 | 53.8 ± 4.1: 46.1 ± 4.1 | 0.813: 0.814 |
| - GC oscillation FP (R:L) | 0.49 ± 0.39: 0.51 ± 0.43 | 0.57 ± 0.5: 0.54 ± 0.38 | 0.096: 0.555 | 0.71 ± 0.97: 0.5 ± 0.3 | 0.48 ± 0.2: 0.44 ± 0.2 | 0.400: 0.333 |
| - GC oscillation SG (R:L) | 2.2 ± 1.26: 2.54 ± 1.08 | 2.5 ± 1.73: 2.61± 0.97 | 0.231: 0.634 | 1.9 ± 0.55: 2.12 ± 0.75 | 1.98 ± 0.6: 2.54 ± 0.5 | 0.932: 0.252 |
| Disability (AOFAS) | ||||||
| - Pain | 10.6 ± 11.1 | 13.33 ± 14.6 | 0.236 | 12.0 ± 12.7 | 9.33 ± 10.3 | 0.546 |
| - Function | 32.2 ± 9.3 | 31.33 ± 9.7 | 0.732 | 34.0 ± 6.5 | 31.2 ± 8.60 | 0.135 |
| - Alignment | 1.4 ± 2.3 | 0.83 ± 2.6 | 0.430 | 1.0 ± 2.8 | 0.1 ± 0.1 | 0.189 |
| - Total | 43.3 ± 19.7 | 46.33 ± 22.7 | 0.473 | 47 ± 19.5 | 40 ± 15.7 | 0.261 |
| Disability (HAQ) | 1.7 ± 0.7 | 1.46 ± 0.71 | 0.084 | 1.50 ± 0.6 | 1.28 ± 0.6 | 0.470 |
Values are presented as mean ± standard deviation.
*Student’s t test.
Abbreviations: AOFAS, American Orthopaedic Foot and Ankle Society ankle-hindfoot scale; FP, frontal plane; GC, gravity center; HAQ, Health Assessment Questionnaire; L, left foot; R, right foot; SG, sagittal plane.
Table 2: Effects of foot orthoses on kinetic, pain, and disability variables.
The results of this randomized controlled trial demonstrated that the effects on the pain and disability after FO use were variable, although there was a trend towards reduced pain and improved foot and ankle disability in the FO group, while the control group tended to show worsened outcomes; however, this did not reach statistical significance.
In RA patients, foot pain and deformities are common, and FO have been considered an adjunct to pharmaceutical treatments [14]. However, previous studies have yielded inconsistent results in terms of the effects of FO on pain and disability [14-16]. Conrad et al. [15] studied functional posted FO in RA patients for three-year period. They found no significant improvements in pain and disability. Despite the large follow-up, their results do not have good external validity, because used unusual sample consisted for older males without foot deformities, while RA is most frequent in females. Another limitation of Conrad and co-works study was a presence of placebo orthoses group. The material used in this placebo orthoses could promote mechanical effects, not establish in the literature and at the same time increase de placebo effect. In contrast, the sample of our study was composed for female and we performed a control group without FO to avoid the placebo response. Woodburn et al. [16] in their clinical trial compared custom design FO with no intervention group. After thirty-months period they found significant improvements on pain and disability. However these findings should be applied only to RA patients with valgus hell deformity. In our study, we included RA patients with foot pain with or without rear and/or forefoot deformities. The expanded scope enhances the generalizability of our results.
Further, Henessy et al. [7], in a recent meta-analysis, found weak evidence for reduced pain upon FO use, and inconclusive findings in terms of disability. Similarly, in our study, we found slight, but nonsignificant, improvements in pain and disability. We speculate that this finding is owing to the fact that the FO were used isolated, with no other concomitant conservative treatment, and could therefore not produce a substantial impact for all systemic complications of RA.
Patients with RA have more musculoskeletal disorders, are more prone to fatigue, and show a greater loss of strength compared to healthy individuals, consequently resulting in instabilities [17]. The moderate economic and low educational levels found in our sample, as revealed by the Health Assessment Questionnaire (HAQ) for RA, may also explain the high levels of deficiency [18]. These clinical and social conditions promote increases in disability that cannot be influenced only by the use of FO, and we speculate that a combination of FO with other conservative treatments such as physical therapy may produce more significant results.
In agreement with Conrad et al. [15], the maintenance of analgesics, anti-inflammatory agents, and anti-depressants used by the subjects in the present study may have interfered with the outcomes and may be responsible for the lack of significance in terms of the post-treatment pain between the groups. However, due to ethical issues, it is impossible to have a true no-treatment group (without drugs). Furthermore, this may also explain the lack of significant reductions in the HAQ score in both groups.
In the present study, a ¾ insole was chosen to improve the adaptation of these devices to the different kinds of women’s shoes, owing to the fact that the main reason given by women to stop using FO has been reported to be that they were not setting to their shoes [10]. Furthermore, the reduction in the length of the FO and the failure to cover the entire surface of the forefoot, which is considered one of the main regions affected in rheumatic feet, may also explain the nonsignificant results [19].
There were others additional limitations in our study. First, there were a high number of dropouts, owing to several reasons, including the surgical procedure, patients moving to another city or traveling during the study period, and loss of the insole. Second, the duration of the intervention was short-term (2 months), and it is possible that improvements in the pain and disability could have been increased upon longer duration of intervention, as in the studies by Woodburn et al. [16] and Cho et al. [19].
Based on the results reported in this study, as well as the findings of the previous reports on the topic, FO do not appear to modify the kinetic variables, but may have a small effect, albeit non-significant, on pain and disability, and these findings may contribute to the definition of best clinical practice. However, further, larger trials are needed to clarify whether the combined use of this device with physical therapy and other conservative treatments can produce significant improvements in pain and disability.
