Research Article - (2015) Volume 0, Issue 0
Objective: We aim to assess the influence of antihistamines as an adjunctive therapy in children with JIA who also have co-existing mild to moderate AR.
Methods: Fifty-two JIA patients with AR were enrolled and consecutively randomized. The control group comprised 26 patients who were treated with methotrexate (MTX) 10-15 mg/m2/week orally for 12 months and enteric-coated diclofenac sodium 0.5-2 mg/kg/day orally for 12 weeks. The test group comprised 26 patients who received adjunctive therapy with oral and intranasal antihistamines for 12 months, in addition to MTX and diclofenac. The responses were evaluated using American College of Rheumatology (ACR) pediatric (Pedi) 30/50/70 criteria, AR score, 27-joint Juvenile Arthritis Disease Activity Score (JADAS-27), and laboratory variables.
Results: At 3 and 6 months follow-up, significantly more patients in the antihistamine treatment group achieved ACR Pedi50 and ACR Pedi70 responses(at 3 months, 73.1% to 19.2%, 38.5% to 7.7%; at 6 months, 96.2% to 53.8%, 76.9% to 19.2%, respectively, all p<0.01). In the antihistamine group the AR score correlated with JADAS-27 at baseline, 3 months and 6 months (r=0.946, r=0.909 and r=0.964, respectively). During 12 months of follow-up, there were significantly fewer JIA flares in the antihistamine group (0.8 ± 0.7 vs. 2.2 ± 1.4, p<0.01).
Conclusions: JIA patients with concurrent AR who receive effective antihistamine treatment for their AR may have better outcomes in terms of JIA control.
Keywords: Juvenile idiopathic arthritis; Allergic rhinitis; Treatment; Outcome; Autoimmune diseases
Juvenile idiopathic arthritis (JIA) is an umbrella term that encompasses all forms of arthritis that begin before the age of 16 years, persist for more than 6 weeks, and are of unknown cause [1]. The worldwide prevalence of JIA varies between 16 and 150 per 100,000 [2]. Abnormalities in the complicated regulatory network of the immune system, including dysfunction of T helper type 1 (Th1), Th17, Th9, and regulatory T cells (Tregs) amongst others, are thought to play a role in the pathogenesis of JIA [1,3,4]. Despite the current availability of potent disease-modifying anti-rheumatic medications, most children still experience a chronic course with prolonged periods of active disease.
Several features have been shown to influence prognosis in JIA, including gender, inflammatory markers and comorbidities [5]. Among the latter, allergic disorders were the most common comorbidities [6]. Allergic rhinitis (AR) is the most common chronic disease in childhood with prevalence in some regions of up to 40% [7]. Pathologic features of AR include elevated serum IgE concentrations, and elevated Th2-type cytokines (IL-4, IL-5, IL-13) [8]. In addition, recent studies have demonstrated that Th17, Th9, and Treg dysfunction is associated with AR [9-11]. As many patients with AR do not seek specialist medical attention, many lack a formal diagnosis or effective management plan. We would hypothesize that, for patients who also have JIA, failure to treat AR may lead to a worse outcome for their arthritis.
JIA and AR are both potential outcomes of immunologic dysregulation, with epidemiological similarities [12]. Allergic conditions have historically been thought to protect against the onset of autoimmune diseases, or to modulate their severity, as a result of the dichotomy of the overactive Th2 lineage associated with allergic manifestations, versus the overactive Th1 response typical of several autoimmune diseases [13]. This Th1/Th2 paradigm, however, conflicts with recent findings on the co-existence of autoimmune disorders and allergies [12]. A growing body of evidence suggests that JIA can be found in association with a variety of allergic diseases [9,11-13]. Raab et al. reported a 14.5% prevalence of AR in their study of adult patients with JIA [6]. Likewise, a 44% prevalence of atopy in systemic-onset JIA patients has been noted by Zhang et al. [13]. These are among many large and relatively recent studies [6,14-16] suggesting that autoimmune and atopic diseases are risk factors for each other.
Several studies focus on Th9, Th17 and Treg activity in the detrimental immune responses of allergic and autoimmune disorders [4,9,17,18]. However, the effect of treatments for the co-occurrence of these disorders, and the efficacy of adjunctive antihistamine treatment for allergic diseases on outcomes in JIA have rarely been demonstrated. Here we report the results of a randomized pilot study to compare the influence and efficacy of adjunctive antihistamine treatment in children with both JIA and AR.
Fifty-two JIA patients with AR were diagnosed by a pediatric rheumatologist and an allergist, respectively, from a pool of 189 patients with JIA at Renji Hospital between March 2010 and March 2014. The diagnosis of JIA was made using the criteria of the International League of Associations for Rheumatology (ILAR), published in 2004 [5]. The diagnosis and severity classification for AR were determined using the criteria from the guideline entitled Allergic Rhinitis and its Impact on Asthma (ARIA) [19]. Exclusion criteria for this study included infectious disease, leukemia, lymphoma, other connective tissue diseases and systemic onset juvenile idiopathic arthritis (SoJIA). For the abnormalities in the innate immune response play a significantly more prominent role in pathogenesis of SoJIA compared to other subtypes of JIA [13]. The study was conducted according to the Declaration of Helsinki and ethics committee approval for this randomized pilot study was obtained at Renji Hospital. Informed consent was obtained from both the parents and children.
Study design
This is a randomized, single-blind pilot study. The evaluation of patient outcomes was performed by a pediatric rheumatologist (H.Y.X., with 5 years of experience in rheumatology) who was blinded to the treatment. Fifty-two patients were consecutively randomized in a 1:1 ratio between control and test (antihistamine) groups. A randomization list was electronically generated according to a complete randomization design with block size of four units; this was managed by the principal investigator (L.J.S., with 4 years of experience in data processing) who was responsible for assigning participants to interventions.
Patients in the control group were treated with a daily oral dose of 0.5-2 mg/kg of diclofenac for 12 weeks and MTX 10-15 mg/m2 weekly for 12 months.
Patients in the antihistamine group were treated with a daily oral dose of 0.5-2 mg/kg of diclofenac for 12 weeks and MTX 10-15 mg/m2 weekly, plus loratadine (5 mg daily for children weighing <30 kg, and 10 mg for those weighing ≥30 kg) and lovocabastine (one spray per nostril twice daily) for 12 months.
All patients were assessed by a pediatric rheumatologist and allergist at baseline and at 3, 6, and 12 months. A standardized data collection protocol was used for all patients. Data collected included age, sex, duration of disease, JIA subtype, AR severity classification, previous medical history, previous and current treatments, side effects of medications, and any individual or family history of allergic diseases (extending to first and second degree relatives). The clinical assessment of each patient included weight, height, joint assessment (number of tender joints, number of swollen joints), and general examinations; global assessments included the physician global assessment of disease activity and patients’/parents’ global assessment of child’s overall well-being using a 10-cm horizontal visual analogue scale (VAS). We also documented scores from the child health assessment questionnaire (CHAQ), JADAS-27 assessment, and, for the assessment of AR, the total symptom score system (T4SS). Blood and urine tests were performed at baseline, 3 months, 6 months and 12 months to determine the following parameters: erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) level, hemoglobin, glucose, transaminases, alkaline phosphatase, gamma-glutamyltransferase, serum creatinine, serum calcium, and creatine kinase. Adherence to medications was monitored by telephone interview including parental or patient pill counts, with pill counts confirmed by an investigator in the clinic (R.R.G., with 3 years of experience in rheumatology).
Study outcomes
JIA responses were scored according to the criteria of ACR Pedi 30, ACR Pedi 50 and ACR Pedi 70 [20]. The JADAS-27 score [21] is computed by assessing the following variables: physician global rating via analog scale; parent/child ratings of well-being and pain, assessed on a 10-cm horizontal VAS; number of active joints, assessed in 27 joints (including cervical spine, elbows, wrists, first to third metacarpophalangeal joints, proximal interphalangeal joints, hips, knees and ankles); and Westergren ESR normalized to a 0-10 scale. The JADAS-27 is calculated as the sum of the scores of its four components, yielding a global score of 0-57.
AR symptoms were assessed using the T4SS with a 0 to 12 scale. AR severity was also assessed by the patient by means of a VAS, from 0 to 10 cm [22]. The AR score is calculated as the sum of the scores of T4SS and VAS, which yields a global score of 0-22.
A JIA relapse was defined as a change in disease status from inactive to active. Patients were defined as having inactive disease if they simultaneously met all of the following criteria [23]: no joints with active arthritis; no fever, rash, serositis, splenomegaly, or generalized lymphadenopathy attributable to JIA; no active uveitis; normal ESR or CRP; no disease activity on the physician’s global assessment. All patients were requested to report any side effects at each visit.
Biochemical measurements
Standard laboratory tests were performed at Renji Hospital. The normal range of ESR is defined as <20 mm/h and CRP as <10 mg/L.
Statistical analysis
Categorical data were expressed by counts or percentages, and compared between different groups by the chi-squared test or Fisher’s exact test. The continuous variables were presented as the mean ± standard deviation, and were analyzed by Student’s t-test or the Mann-Whitney U-test as appropriate. The association between JADAS-27 and AR score in the antihistamine group at baseline, 3 and 6 months was evaluated using Spearman’s rank correlation. A p-value of <0.05 was considered statistically significant. All analyses were performed using the SPSS software version 13.0 (SPSS Inc.; Chicago, IL, USA).
Patient enrollment was carried out between March 2010 and March 2014 at the Renji Hospital and all patients completed the 12-month follow-up. The control group consisted of 26 patients, 17 males and 9 females, with mean age 11 years (range 6-15 years). The antihistamine group consisted of 26 patients, 20 males and 6 females, with mean age 11 years (range 6-14 years). The baseline characteristics of the enrolled patients are shown in Table 1 (Demographics and characteristic of JIA patients with AR at the baseline). The JIA ACR Pedi core components, such as physician’s global assessment , patients’/parents’ global assessment of child’s overall well-being VAS,ESR, number of active joints, number of restricted joints, number of painful joints, parent global assessment of child’s pain VAS and CHAQ, did not show any significant diference at baseline. The knee, ankle, wrist, and sacroiliac were the most frequently involved joints in our study and marrow edema was found in magnetic resonance imaging (MRI) (Figure 1 Radiographic findings of frequently involved joints).
| Characteristic | Control group (n=26) | Antihistamines group (n=26) | p value |
|---|---|---|---|
| Gendera (boys) | 17/26 (65.4%) | 20/26 (76.9%) | 0.358 |
| Current ageb, years | 11 (6~15) | 11 (6~14) | 0.803 |
| JIA Subtypesa | 0.482 | ||
| Oligoarthritis | 2/26 (7.7%) | 2/26 (7.7%) | |
| Polyarthritis | 5/26 (19.2%) | 2/26 (7.7%) | |
| Enthesitis-related arthritis | 19/26 (73.1%) | 22/26 (84.6%) | |
| AR severity classificationa | 0.358 | ||
| Mild | 20/26 (76.9%) | 17/26 (65.4%) | |
| Moderate | 6/26 (23.1%) | 9/26 (34.6%) | |
| Disease characteristics | |||
| CRP, mg/Lc | 11.6 ± 10.2 | 8.0 ± 8.5 | 0.172 |
| ESR, mm/hc | 33.5 ± 24.5 | 24.5 ± 22.6 | 0.179 |
| Physicians’ VASc | 5.3 ± 1.0 | 4.9 ± 1.1 | 0.117 |
| Patients’ VASc | 3.7 ± 1.1 | 3.4 ± 0.86 | 0.326 |
| Number of active jointsc | 4.0 ± 2.2 | 3.7 ± 2.5 | 0.683 |
| Number of restricted jointsc | 2.2 ± 1.9 | 1.7 ± 1.7 | 0.289 |
| CHAQ scorec | 0.9 ± 0.4 | 0.9 ± 0.3 | 0.926 |
| No. of painful jointsc | 2.5±1.8 | 2.3±2.0 | 0.715 |
| Parent global assessment of child’s pain VASc | 4.5±2.8 | 3.6±2.8 | 0.26 |
CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; physicians’ VAS, physician’s global assessment of disease activity on a 10-cm visual analogue scale; patients’ VAS, patients’/parents’ global assessment of child’s overall well-being on a 10-cm visual analogue scale ; CHAQ, childhood health assessment questionnaire.
aFrequency/total, between group comparisons: Chi-square test or Fisher’s exact test.
bMedian and interquartile range, between group comparison: Mann-Whitney U test.
cMedian ± standard deviation, between group comparison: Student’s t-test.
*p< 0.05 indicates a significant difference between the different groups.
Table 1: Demographics and characteristic of JIA patients with AR at the baseline.
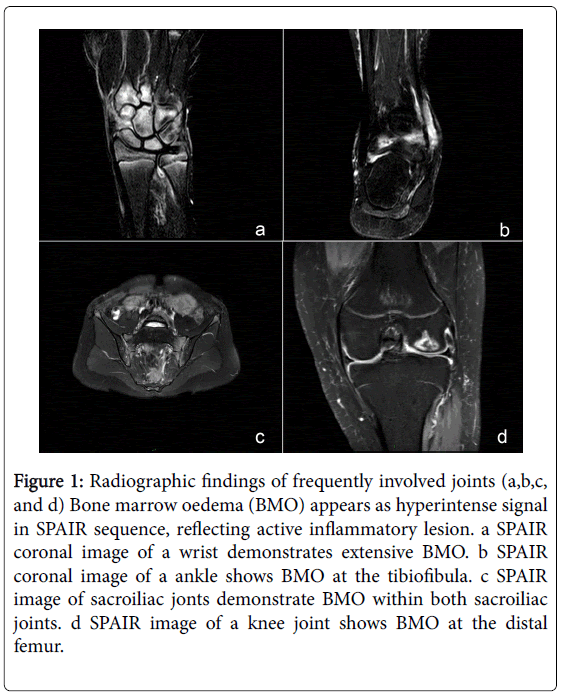
Figure 1: Radiographic findings of frequently involved joints (a,b,c, and d) Bone marrow oedema (BMO) appears as hyperintense signal in SPAIR sequence, reflecting active inflammatory lesion. a SPAIR coronal image of a wrist demonstrates extensive BMO. b SPAIR coronal image of a ankle shows BMO at the tibiofibula. c SPAIR image of sacroiliac jonts demonstrate BMO within both sacroiliac joints. d SPAIR image of a knee joint shows BMO at the distal femur.
After 3 months of treatment, significantly fewer patients in the antihistamine group had ESR values >20 mm/h compared with the control group (15.4% to 42.3%, p = 0.032). The patients treated with antihistamines also had a markedly higher frequency of ACR Pedi 30, ACR Pedi 50, ACR Pedi 70 responses (80.8% to 34.6%, 73.1% to 19.2%, 38.5% to 7.7%, respectively, all p < 0.05) than the control group, which demonstrated a significant additive value of antihistamine treatment on JIA outcomes. At 6 months, 20 of 26 patients in the control group reached ACR Pedi30 (76.9%), 14 reached ACR Pedi50 (53.8%), and 5 reached ACR Pedi70 (19.2%). By contrast, in the antihistamine group, 25 of 26 patients achieved ACR Pedi30 and ACR Pedi50 (96.2%), and 20 reached ACR Pedi70 (76.9%). Comparison between the two groups indicated a significantly higher rate of ACR Pedi50, ACR Pedi70 responses in the treatment arm compared with the control group (p < 0.001) (Figure 2 Laboratory features and clinical assessment of JIA patients with AR at 3 months and 6 months following enrollment).
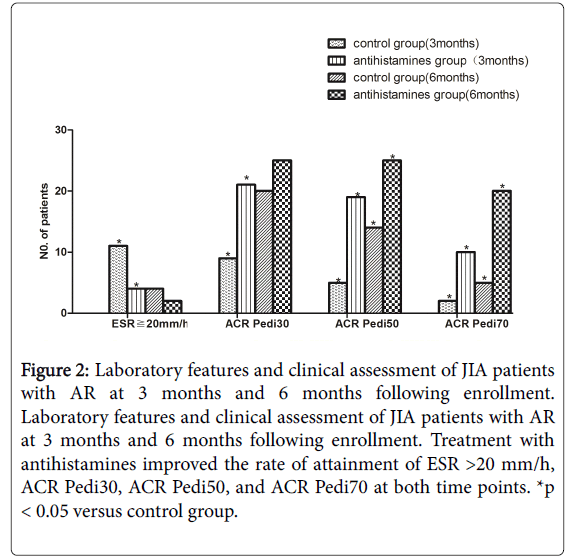
Figure 2: Laboratory features and clinical assessment of JIA patients with AR at 3 months and 6 months following enrollment. Laboratory features and clinical assessment of JIA patients with AR at 3 months and 6 months following enrollment. Treatment with antihistamines improved the rate of attainment of ESR >20 mm/h, ACR Pedi30, ACR Pedi50, and ACR Pedi70 at both time points. *p < 0.05 versus control group.
To determine whether the co-occurrence of AR among patients with JIA was associated with the disease activity of JIA, we assessed the T4SS and VAS for AR (i.e., AR score) and the JADAS-27 score. We evaluated the correlation between JADAS-27 and the AR score in the antihistamine group at baseline, and found that the AR score was positively associated with JADAS-27 (r = 0.946, p < 0.001). Following antihistamine treatment for AR, which reduced the AR score, there was a similar reduction in the JADAS-27 score at the 3-month follow-up (r = 0.909, p < 0.001) and at the 6-month follow-up (r = 0.964, p < 0.001), as shown in Figure 3 (Relationship between AR score and JADAS-27 in patients treated with antihistamines at baseline, 3 months and 6 months).
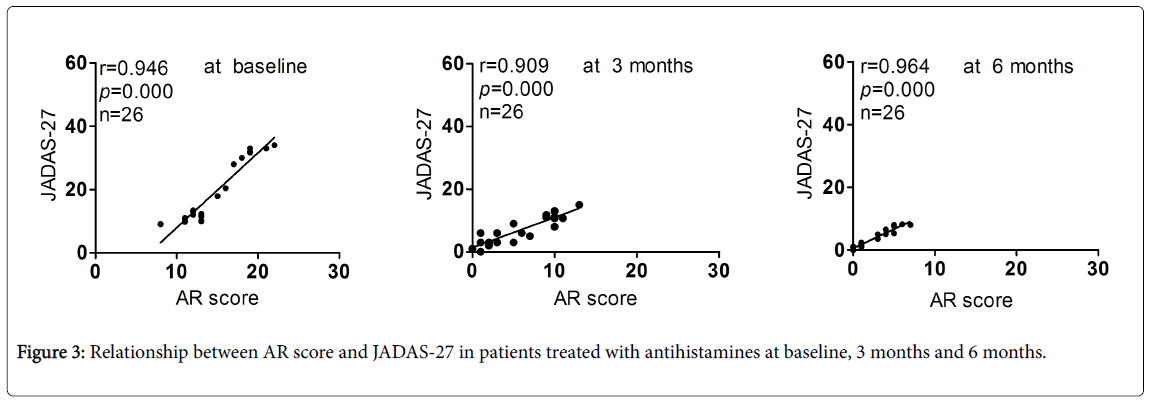
Figure 3: Relationship between AR score and JADAS-27 in patients treated with antihistamines at baseline, 3 months and 6 months.
During the 12-month follow-up, the number of JIA flares in patients in the antihistamine group was significantly lower than that of the control group (0.8 ± 0.7 vs. 2.2 ± 1.4, p = 0.004).
This randomized, single-blind pilot study of 52 patients with both JIA and AR adds support to previous studies that suggested these conditions are not mutually exclusive. Treatment of AR by oral and intranasal antihistamines is associated with improvements in JIA outcomes measured by the ACR Pedi30/50/70 compared to standard JIA treatment alone. JIA patients with co-existing AR at enrollment to the study were matched for disease status, with all being in active stage. Patients receiving regular oral and intranasal antihistamine therapy in addition to standard JIA treatment were significantly more likely to achieve ACR Pedi30/50/70 scores at 3 months and 6 months compared to patients receiving standard therapy alone. Furthermore, in the antihistamine treatment group we demonstrated a correlation between the AR score, measured by T4SS and VAS, and disease activity in JIA, as measured by the JADAS-27. To the best of our knowledge, this is previously unreported in the literature, and suggests that therapeutic intervention with antihistamines for patients with both AR and JIA may be beneficial for JIA control.
At a mechanistic level, there are many common immune pathways featuring Th9, Th17, and Treg dysregulation that may be shared between AR and JIA. Similar underlying genetic tendencies and environmental factors may also be implicated. The recently described Th9 cell subset characteristically produces IL-9, an important mediator of allergy that was originally classified as a Th2-derived cytokine. Th9 cells, in concert with Th2 cells, drive the pathogenesis of type 2 inflammatory diseases [4]. Recent studies have indicated that Th9 cells and IL-9 are also closely implicated in autoimmune diseases [24], as demonstrated by murine models of Th1/Th17-driven human autoimmune disease. IL-9 also significantly enhances IL-17A production by cultured human peripheral blood mononuclear cells or CD4+ T cells in autoimmune diseases [25].
Recently, patients with JIA have been shown to have high levels of IL-17 in active, inflamed joints, and increased numbers of IL-17-producing T cells. This induces the production of other interleukins and matrix metalloproteinases that are all involved in joint damage [26]. As well as this role in JIA, Th17 cells, which produce IL-17, also appear to contribute to atopy by promoting IgE class-switch recombination in B cells through stimulation of ε germline transcripts [27]. Since AR is a prevalent yet underappreciated inflammatory disorder [8], it is possible that prolonged untreated AR-associated inflammation, with high IL-17, may exacerbate JIA in patients who have both conditions.
Many studies have demonstrated that Treg cells play a pivotal role in the maintenance of immune tolerance, thus helping to prevent autoimmune diseases and allergy [28,29]. T-cell derived pro-inflammatory cytokine levels in the affected joints of JIA patients are high, while Treg cells and anti-inflammatory cytokines (IL4, IL-10 and TGF-β) are reduced in JIA [5]. Furthermore, Treg function has been shown to be impaired in JIA as synovial fluid Tregs are unable to suppress T effector cells found in the joint. These abnormalities also correlate with disease severity [30]. Likewise, Treg cells that produce IL-10 suppress Th2 lymphocyte responses to allergens in health, whereas this inhibition is attenuated in allergic disorders [8]. With regard to AR, recent studies have demonstrated that peripheral blood mononuclear cells from affected patients have significantly fewer Foxp3+ lymphocytes and decreased Foxp3 mRNA expression; Tregs from atopic patients also have less suppressive activity compared with non-atopic groups [18,31]. Hence, there are plausible immunological explanations for why co-occurrence of JIA and AR should be associated with less favorable JIA control.
As described above, JIA and AR may influence each other by common dysregulated immune pathways. Therefore, in order to improve the outcome of JIA patients who also have AR, antihistamines can be considered as adjuncts to JIA therapy. We have confirmed the positive response to AR treatment in this patient group, which not only controls the AR, but also reduces the risk of relapse of the primary disease. Furthermore, our study suggests that antihistamine treatment used as an adjunct to therapy may be beneficial to JIA control. The limitations of this randomized, single-blind pilot study relate to the relatively small group sizes and to our inability to detect and quantify the immune effector cells and cytokine activity that may underlie the responses to AR treatment. Larger trials that incorporate laboratory assessment of these factors would add further weight to the findings discussed here, and will be the focus of further study.
In conclusion, we have shown that the addition of antihistamine treatment for AR is effective in reducing JIA disease activity, leading to improved clinical outcomes. Antihistamine treatment for concurrent AR may therefore be an effective treatment strategy for JIA.
Each author’s contribution
RR Guo: Contribution to execution of study, collection of data, analysis and interpretation of data and drafting and revising the article.
LF Cao: Contribution to conception and design of the study, acquisition of funding, analysis of data, revising the article and supervision of the research group.
XM Kong: Contribution to reading, revising the article and approval of the final version.
HY Xue: Contribution to collection of data, analysis and interpretation of data, revising the article.
XL Li: Contribution to collection of data, reading and analysis of data, and revising it critically for important intellectual content.
LJ Shen: Contribution to collection of data, execution of study and analysis of data, and revising it critically for important intellectual content.
The work was supported by a grant from the Second Major Research Project of the Three Years’ Shanghai Traditional Chinese Medicine Career Development Action Plan of Shanghai Health Bureau (Project Number: ZYSNXD-CC-ZDYJ030).
