Case Report - (2015) Volume 0, Issue 0
A case of rheumatoid thumb carpometacarpal (CMC) arthritis with advanced osteolysis is reported. Although CMC joint arthrodesis was performed, bone union was not achieved, and pain and instability persisted. Therefore, first and second metacarpal bone fusion was performed with satisfactory results. While CMC joint arthrodesis or arthroplasty is typically performed, first and second metacarpal bone fusion appears to be a useful treatment option when there is marked osteolysis.
Keywords: Rheumatoid arthritis; First carpometacarpal joint; First and second metacarpal bone fusion
If the degree of osteolysis is mild in rheumatoid thumb carpometacarpal (CMC) arthritis, patients are treated with CMC joint arthrodesis or arthroplasty. However, if there is severe or advanced osteolysis, these procedures are difficult to perform. A case in which first and second metacarpal bone fusion was performed in a patient with severe osteolysis is described.
The patient was a 68-year-old woman with chief complaints of right hand finger rheumatoid deformities, specifically extensor tendon dislocation of the middle, ring, and little fingers, ulnar deviation of the ring and little fingers, and pain and instability of the thumb CMC joint. X-ray showed many collapsed carpal bones, dislocation of the metacarpophalangeal (MP) joint in the index, middle, ring, and little fingers, and marked osteolysis of the CMC joint (Figure 1). The patient had been taking methotrexate and adalimumab. Ulnar head resection, or the so-called “Darrach method,” had been performed 3 months previously for right wrist ulnar pain. Silicone implants were inserted into the index, middle, ring, and little fingers, abductor digiti minimi (ADM) was resected, crossed intrinsic transfer of the ring finger was performed to the radial side of the little finger MP joint, and the extensor tendons of the middle, ring, and little fingers were centralized.
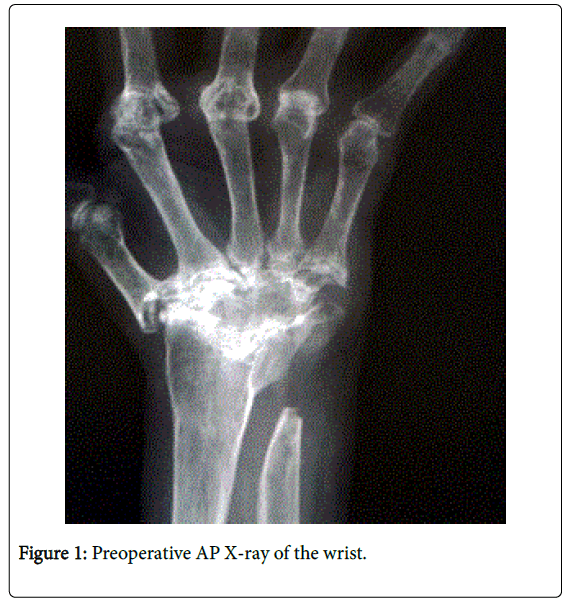
Figure 1: Preoperative AP X-ray of the wrist.
For the thumb CMC joint, the cartilage was scraped and fixed using a compression screw. Extensor tendon dislocation of the middle, ring, and little fingers, and ulnar deviation of the fingers were improved 2 months postoperatively. However, bone union was not achieved at the thumb CMC joint, and the screw began to protrude. In the repeat surgery, the screw was replaced, and Kirschner wire (K-W) was used for additional fixation.
However, bone healing was still not achieved, and the K-W began to protrude. Additionally, tenderness in the thumb CMC joint, as well as pain during thumb abduction and pinch movement, continued. Therefore, first and second metacarpal bone fusion was performed using an iliac bone graft 3 months after the initial surgery. Specifically, the sides of the first and second metacarpal bones were shaved, the cancellous bone was exposed, and the iliac bone was inserted and fixed with a compression screw (Figure 2). At 70 months post-operation, there was satisfactory flexion, extension, and abduction of the thumb, a certain degree of opening at the first web space, no pain at the CMC joint, and an improvement in pinch strength from 1 kg preoperatively to 2.6 kg postoperatively (Figure 3). Plain X-ray and CT images also showed bone union (Figure 4).
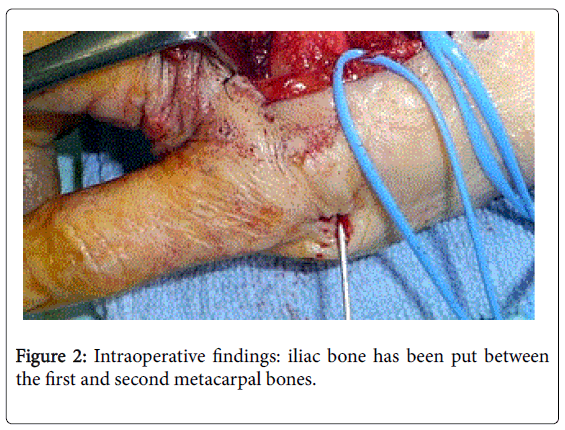
Figure 2: Intraoperative findings: iliac bone has been put between the first and second metacarpal bones.
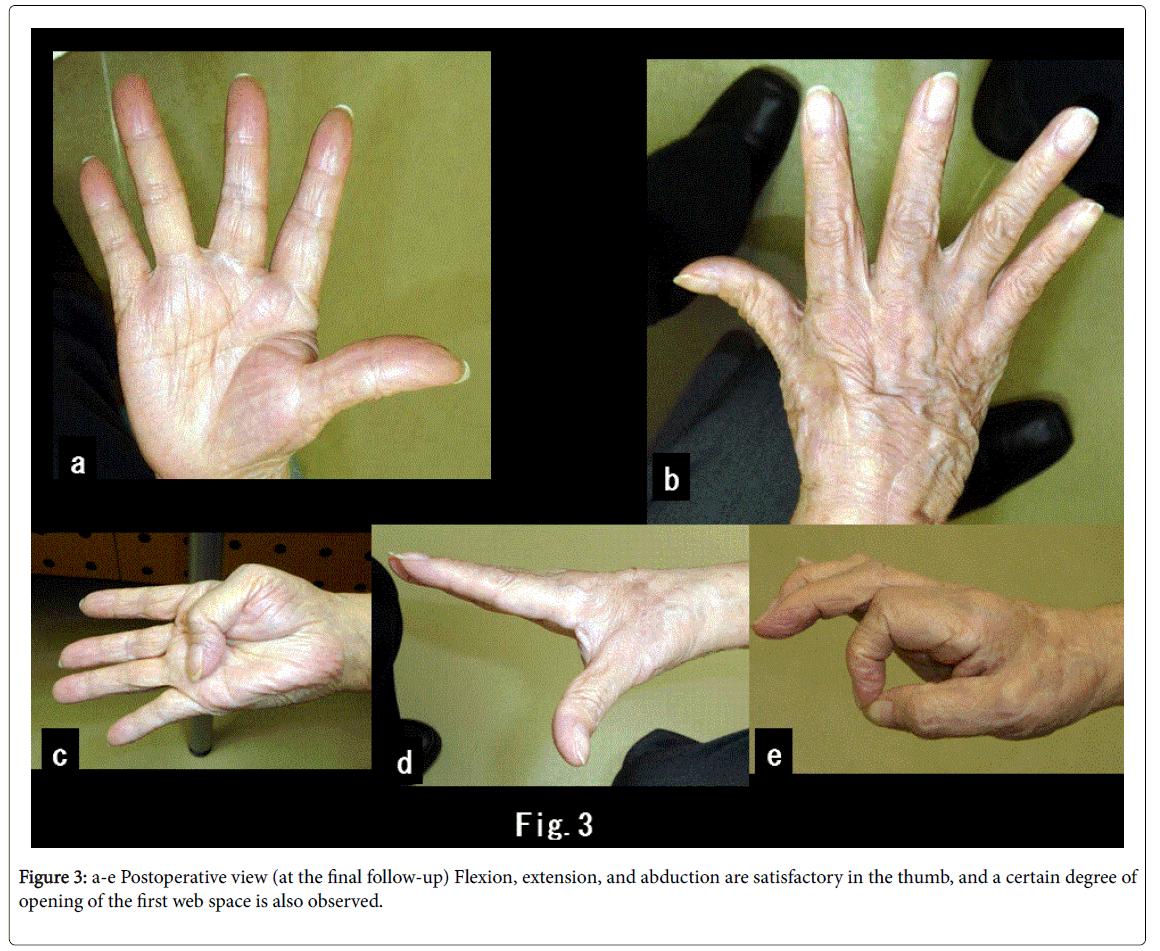
Figure 3: a-e Postoperative view (at the final follow-up) Flexion, extension, and abduction are satisfactory in the thumb, and a certain degree of opening of the first web space is also observed.
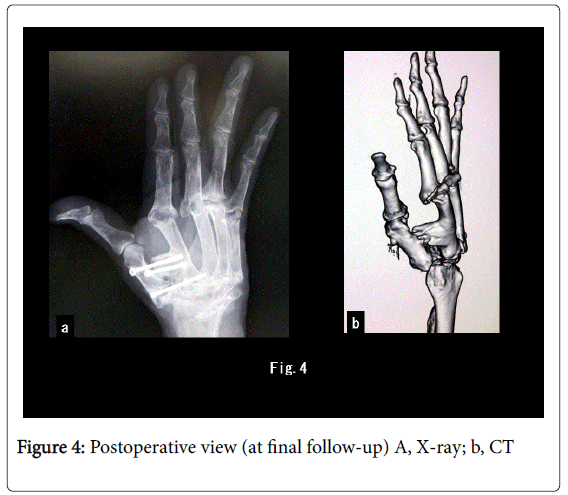
Figure 4: Postoperative view (at final follow-up) A, X-ray; b, CT
For rheumatoid thumb deformities, the classification method described by Nalebuff is well known [1]. The patient in the present case report corresponded to Type 3 of this classification. Type 3 is a deformity that initially appears at the thumb CMC joint where the first metacarpal bone shows an adduction deformity and the thumb shows a swan-neck deformity. In the present case, however, the patient only had a mild swan-neck deformity and no functional disorder at the MP and interphalangeal (IP) joints. The CMC joint had severe osteolysis, and the first metacarpal bone was shortened, subluxated, and in contact with the radius. For the treatment of a Type 3 CMC joint, procedures such as joint arthrodesis, artificial joint procedures, [2,3] and arthroplasty [4,5] are used. Each procedure has its advantages and disadvantages. For example, the joint arthrodesis fixes the thumb in the abduction position, but doing so restricts adduction movement. Moreover, the other two joints (MP and IP) involved in the arthrodesis procedure must be in relatively good form. In the artificial joint procedure, there are issues of repeat surgery [2] and synovitis of silicone products.3 In arthroplasty, there are issues such as persisting pain, [4] decreased pinch strength, and unclear long-term outcome [4,5]. In the current case, CMC joint arthrodesis was performed, but bone healing was not achieved.
In situations where severe bone deformation and osteolysis are present, where the trapezium is destroyed, and where the first metacarpal bone is shortened due to the proximity of the first metacarpal bone and radius, CMC joint arthrodesis and arthroplasty are typically difficult to perform. In arthroplasty, it is difficult to maintain the first web space and to restrict its movements, and if this restriction is strong, thumb adduction occurs. However, if first and second metacarpal bone fusion is performed, the first web space can be maintained, and thumb adduction can be prevented. In addition, it is easier to achieve bone healing due to the large recipient area of bone graft. If the rheumatoid arthritis is properly controlled, as long as bone union is completed and no subsequent correction losses occur, long-term pain relief can be anticipated postoperatively.
First and second metacarpal bone fusion appears to be a useful treatment option in rheumatoid arthritis patients with severe destruction of the thumb CMC joint.
