Research Article - (2014) Volume 3, Issue 1
Background: Blockade of inflammatory cytokines such as IL-1β, IL-6, and TNF-α inhibits the progression of joint damage in hands and feet in Rheumatoid Arthritis (RA). However, it has been recently reported that TNF inhibitors have little effect on the large weight-bearing joints once joint destruction has started. On the other hand, intraarticular injection of high-molecular-weight sodium Hyaluronate (HA) prevents cartilage degeneration in the large weight-bearing joints in osteoarthritis.
Objectives: We examined the effects of combinations of cytokine inhibitor and HA on the expression of ADAMTS (a disintegrin and metalloproteinase with thrombospondin motifs), MMPs (matrix metalloproteinases), and RANKL (receptor activator of nuclear factor κB ligand), which all play important roles in joint damage, in human RA fibroblastlike synoviocytes (RA-FLS) and chondrocytes.
Methods: RA-FLS and chondrocytes were cultured for 24 h in the presence of synovial fluid from active RA patients (CRP>12 mg/dL, n=5) with or without HA, IL-1 receptor antagonist, soluble TNF receptor-Fc (etanercept), and anti-IL-6 receptor antibody (tocilizumab). After culture, the levels of ADAMTS-4, MMP-3, and RANKL mRNA were measured by real-time PCR.
Results: RA synovial fluids induced ADAMTS-4,MMP-3, and RANKL mRNA expressions in RA-FLS and chondrocytes. Cytokine inhibitors partially inhibited ADAMTS-4,MMP-3, and RANKL mRNA expressions, showing that several cytokines are involved in the expression of joint destruction factors. The RA synovial fluids contained IL-1β, IL-6, soluble IL-6 receptor, and TNF-α. HA also partially inhibited ADAMTS-4,MMP-3, and RANKL mRNA expressions. Use of each cytokine inhibitor in combination with HA inhibited the production of these factors further than monotherapy with either.
Conclusions: Our results indicate that HA may be useful in preventing joint damage in large weight-bearing joints in RA patients. Furthermore, the concomitant use of cytokine inhibitors and HA might be of greater benefit for preserving cartilage function in RA patients.
Keywords: High-molecular-weight hyaluronic acid; IL-1β; IL-6; TNF-α; Fibroblast-like synoviocytes; Chondrocytes
Rheumatoid Arthritis (RA) is characterized by persistent inflammation of the synovial membranes, and many types of cells are activated by the inflammatory cytokines present in the synovial fluid. RA patients develop multiple systemic symptoms, particularly joint inflammation and destruction of bone and articular cartilage, with some patients suffering permanent disability [1]. The two components of joint damage appear to be consequences of pathogenic processes: (1) Bone erosion is mediated primarily by osteoclasts, which are activated by pro-inflammatory cytokines, and their destructive action is not counterbalanced by bone formation [2,3]; and (2) breakdown of the cartilage matrix is mediated by matrix degradation and inhibition of matrix synthesis induced by cytokines [4,5].
Pro-inflammatory cytokines such as IL-1β, TNF-α and IL-6 play key roles in the pathogenesis of RA. These cytokines are abundant in the synovial fluid of affected joints, and anti-cytokine therapy greatly improves the signs and symptoms of RA [6-8] and prevents progression of joint destruction as assessed radio graphically [9-11]. Radiographic assessment of joint damage using the modified Sharp score is mainly restricted to small joints in the hands and feet; however, because radiographic damage in large weight-bearing joints, such as the hips, knees, and ankles, is strongly associated with walking disability and is an important determinant of functional capacity in patients with RA [6,7], assessment of the extent of radiographic damage in these large joints is essential. Seki et al. [12] reported that in all hip and knee joints with moderate to advanced pre-existing damage radiographic progression continued even if patients received TNF-α blockade therapy.
Intra-articular injection of Hyaluronate (HA) is now widely used in the treatment of Osteoarthritis (OA). The main mechanism through which HA prevents cartilage destruction and disease progression is thought to be its action in maintaining the viscoelastic properties of the synovial fluid [13]. In addition to this, we and others have reported that HA down-regulates the expressions of MMP (Matrix Metalloproteinase) and ADAMTS (A Disintegrin And Metalloproteinase With Thrombospondin Motifs), which are involved in the degradation of cartilage, and RANKL (Receptor Activator of NF-κBLigand), which is related to osteoclastogenesis, induced in synovial fibroblasts and chondrocytes by pro-inflammatory cytokines [14-16]. Moreover, intraarticular injection of HA is approved in Japan to reduce knee-joint pain in RA patients [17].
From these lines of evidence, we hypothesized that HA used concomitantly with a cytokine inhibitor may be beneficial for preventing joint destruction in weight-bearing joints of RA patients. In order to prove this hypothesis, we examined the combination effect of cytokine inhibitors and HA on expression of MMPs, ADAMTS, and RANKL induced in synovial fibroblasts and chondrocytes by synovial fluids of RA patients (RA-SF).
Reagents
Human soluble IL-6 receptor (sIL-6R) and tocilizumab (humanized anti-human IL-6 receptor antibody, TCZ) was prepared in our laboratories [18]. Recombinant TNF-α-receptor (p75)-Fcfusion protein (etanercept, ETN) was purchased from Wyeth (Munster, Germany). IL-1 receptor antagonist (IL-1Ra) was purchased from R&D Systems (Minneapolis, MN, USA). Human IgG was purchased from Sigma-Aldrich (St Louis, MO, USA). High-molecular-weight 2700 kDa HA (Suvenyl®), which is produced by a fermentation method using Streptococcus equi and prepared as a formulation with a concentration of 10 mg/mL, was obtained from Chugai Pharmaceutical (Tokyo, Japan).
Synovial fluids of RA patients
Synovial fluids of RA patients (RA-SF) were obtained from ProteoGenex (Culver City, CA, USA). A total of 5 patients with RA were recruited for the study. Prior to participation, written informed consent was obtained from all subjects. All studies were performed in accordance with the Declaration of Helsinki.
Cytokine concentrations of RA-SF were measured by Procarta Cytokine Assay Kit (Affymetrix, Santa Clara, CA, USA). Soluble IL-6 receptor concentration was measured by human IL-6 receptor alpha Quantikine ELISA Kit (R&D Systems).
Cell culture
Human fibroblast-like synoviocytes from RA patients (RA-FLS) were purchased from Cell Applications (San Diego, CA, USA). RA-FLS were cultured using synoviocyte growth medium (Cell Applications). Human articular chondrocytes were purchased from Cell Applications and maintained in chondrocyte growth medium (Cell Applications).
RA-FLS and chondrocytes (1×105 cells/0.2 mL/well) were seeded into 48-well plates and cultured for 24-48 h until subconfluent. Cells were then cultured for 24 h with RA-SF (diluted to various concentrations with the growth medium for each cell type) in the presence of TCZ (10-300 μg/mL), ETN (10-300 μg/mL), IL-1Ra (10- 300 μg/mL), or HA (0.1-3 mg/mL).
Quantitative real-time PCR
Total RNA was extracted using an RNeasy kit (Qiagen, Valencia, CA, and USA). Synthesis of cDNA was performed using an OmniscriptRT kit (Qiagen) with random 9-mer primers (TaKaRa, Shiga, Japan) according to the manufacturer’s protocol. Quantitative real-time PCR was performed by running a TaqMan gene expression assay (Applied Biosystems, Foster City, CA, USA), targeting human RANKL, MMP- 3, ADAMTS-4, and glyceraldehyde 3-phosphate dehydrogenase (GAPDH), on an ABI PRISM 7500 system (Applied Biosystems) according to the manufacturer’s protocol.
Statistical analysis
Statistical significances were estimated by the unpaired t-test and Dunnett’s multiple comparison test using a software package (SAS Institute Japan, Tokyo, Japan), with the significance level set to 5%.
Effect of RA-SF on RANKL, MMP-3, and ADAMTS-4 expression
Firstly we examined the effect of RA-SF on mRNA expression of MMP-3, RANKL, and ADAMTS-4 in RA-FLS and chondrocytes. RAFLS were cultured with diluted RA-SF:medium dilutions of 1:15 and 5:15 for 24 h. RA-SF induced RANKL and MMP-3 but not ADAMTS-4 in RA-FLS, and induced MMP-3 and ADAMTS-4 but not RANKL in chondrocytes in a concentration-dependent manner (Figure 1). From these results, we used the RA-SF:medium dilution of 5:15 of RA-SF in following experiments.
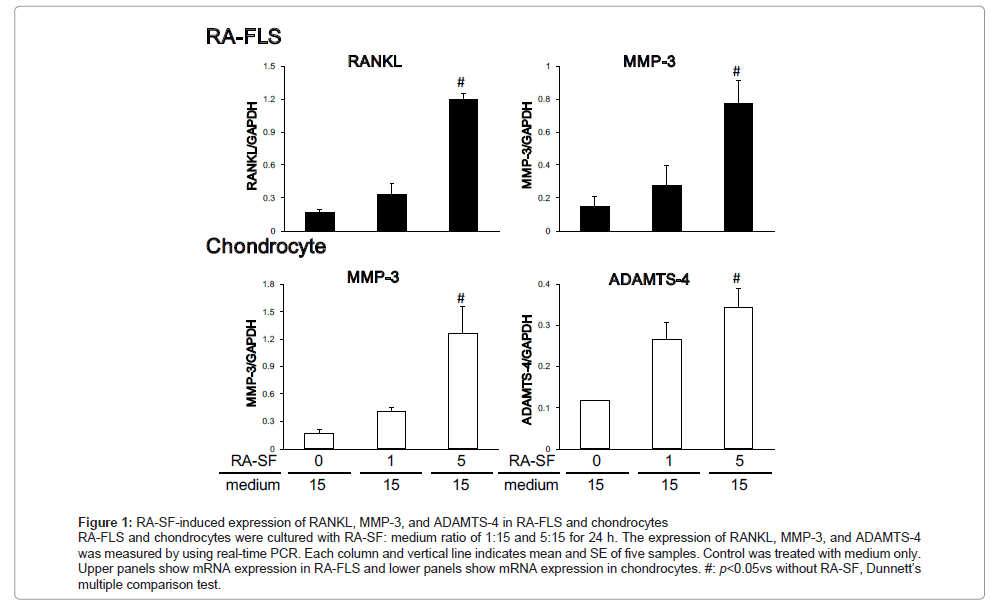
Figure 1:RA-SF-induced expression of RANKL, MMP-3, and ADAMTS-4 in RA-FLS and chondrocytes RA-FLS and chondrocytes were cultured with RA-SF: medium ratio of 1:15 and 5:15 for 24 h. The expression of RANKL, MMP-3, and ADAMTS-4 was measured by using real-time PCR. Each column and vertical line indicates mean and SE of five samples. Control was treated with medium only. Upper panels show mRNA expression in RA-FLS and lower panels show mRNA expression in chondrocytes. #: p< 0.05vs without RA-SF, Dunnett’s multiple comparison test.
Effect of cytokine inhibitors and HA
We examined the impact of the cytokine inhibitors on the RA-SFinduced RANKL, MMP-3, and ADAMTS-4 expressions in RA-FLS and chondrocytes. The inhibitors of IL-6 (TCZ), TNF-α (ETN), and IL-1 (IL-1Ra) suppressed RA-SF-induced RANKL and MMP-3 expressions in RA-FLS, and suppressed MMP-3 and ADAMTS-4 expressions in chondrocytes in a dose-dependent manner (Figure 2). With each inhibitor, the inhibitory effect plateaued at 100 μg/mL.
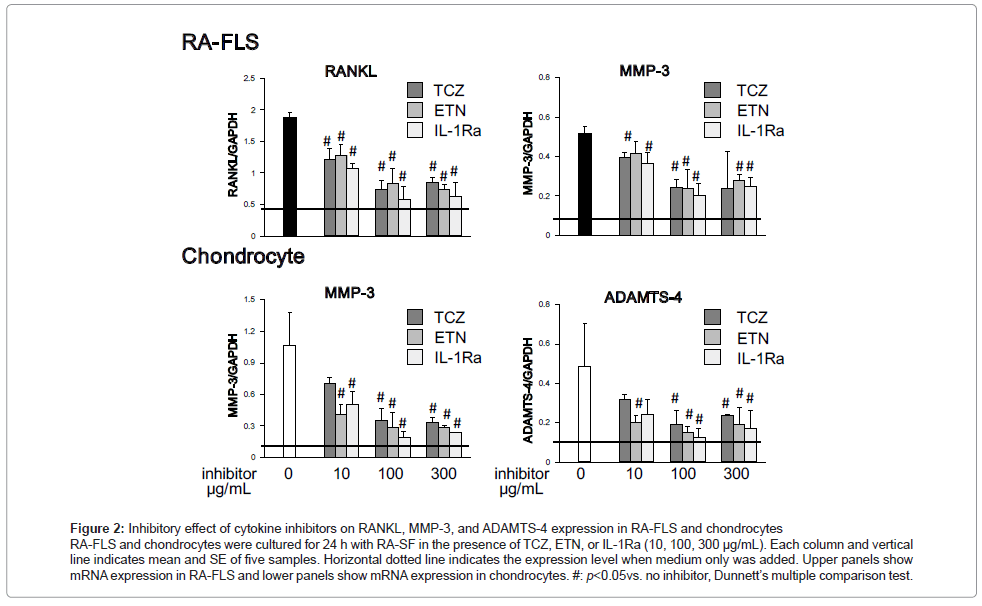
Figure 2: Inhibitory effect of cytokine inhibitors on RANKL, MMP-3, and ADAMTS-4 expression in RA-FLS and chondrocytes RA-FLS and chondrocytes were cultured for 24 h with RA-SF in the presence of TCZ, ETN, or IL-1Ra (10, 100, 300 μg/mL). Each column and vertical line indicates mean and SE of five samples. Horizontal dotted line indicates the expression level when medium only was added. Upper panels show mRNA expression in RA-FLS and lower panels show mRNA expression in chondrocytes. #: p<0.05vs. no inhibitor, Dunnett’s multiple comparison test.
We then measured the concentrations of sIL-6R, IL-6, TNF-α, and IL-1β in RA-SF. We detected sIL-6R, IL-6, and TNF-α in all five samples, but IL-1β was below the limit of detection in two of the five samples (limit of detection: 15.8 pg/mL)
(Table 1).
Next, we examined the inhibitory effect of HA on RA-SF-induced RANKL, MMP-3, and ADAMTS-4 in RA-FLS and chondrocytes. HA inhibited RA-SF-induced RANKL and MMP-3 expressions in RA-FLS, and inhibited RA-SF-induced MMP-3 and ADAMTS-4 expressions in chondrocytes in a dose-dependent manner (Figure 3). The suppressive effect of HA plateaued at 1 mg/mL (data not shown).
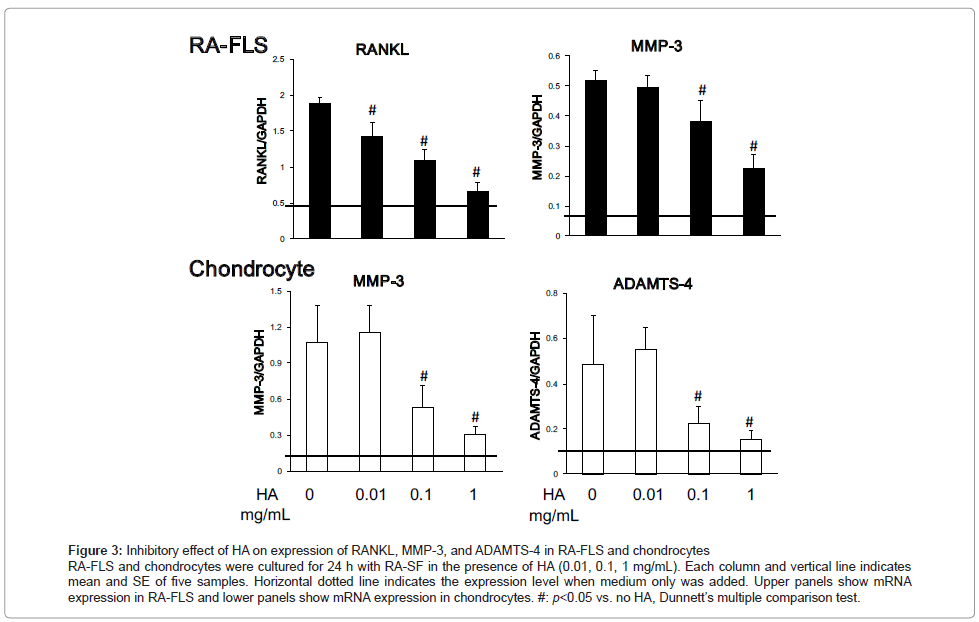
Figure 3: Inhibitory effect of HA on expression of RANKL, MMP-3, and ADAMTS-4 in RA-FLS and chondrocytes RA-FLS and chondrocytes were cultured for 24 h with RA-SF in the presence of HA (0.01, 0.1, 1 mg/mL). Each column and vertical line indicates mean and SE of five samples. Horizontal dotted line indicates the expression level when medium only was added. Upper panels show mRNA expression in RA-FLS and lower panels show mRNA expression in chondrocytes. #: p<0.05 vs. no HA, Dunnett’s multiple comparison test.
Combination effect of HA and cytokine inhibitor
Finally, we examined the combination effect of cytokine inhibitor plus HA (Figure 4). Compared with cytokine inhibitors only, the combination of each cytokine inhibitor and HA more potently reduced the expression of RANKL in RA-FLS, and the expressions of MMP- 3 and ADAMTS-4 in chondrocytes. Interestingly, RANKL expression was reduced by the combination treatment to below the non-stimulated level. On the other hand, MMP-3 expression in RA-FLS was not further decreased by the addition of HA.
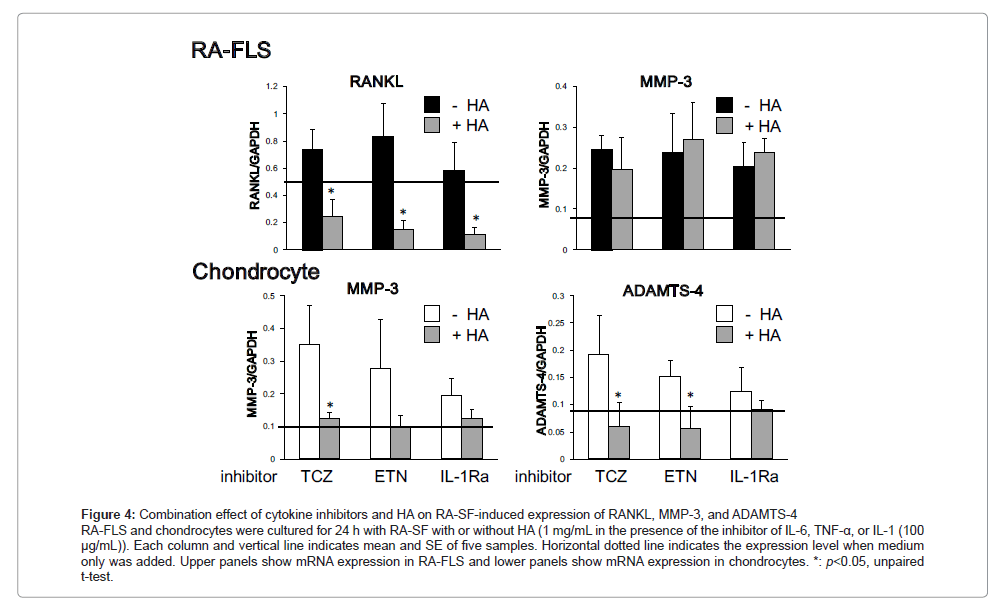
Figure 4: Combination effect of cytokine inhibitors and HA on RA-SF-induced expression of RANKL, MMP-3, and ADAMTS-4 RA-FLS and chondrocytes were cultured for 24 h with RA-SF with or without HA (1 mg/mL in the presence of the inhibitor of IL-6, TNF-α, or IL-1 (100 μg/mL)). Each column and vertical line indicates mean and SE of five samples. Horizontal dotted line indicates the expression level when medium only was added. Upper panels show mRNA expression in RA-FLS and lower panels show mRNA expression in chondrocytes. *: p<0.05, unpaired t-test.
In the present study, we examined the effects of RA-SF on mRNA expression of MMP-3, ADAMTS-4, and RANKL in RA-FLS and chondrocytes. We further studied the inhibitory effects of cytokine inhibitors and HA on these expressions.
Joint damage such as bone destruction and cartilage degeneration is a major contributor to disability in RA patients [19]. In clinical trials, joint damage is routinely assessed using validated radiographic scores [20-22]. In the Sharp score and its modifications, bone destruction is reflected in the erosion score and cartilage degeneration is reflected in the joint-space narrowing score [22-24]. MMP and ADAMTS are enzymes which cleave cartilage matrix, so overproduction of these enzymes induces cartilage degeneration [25]. On the other hand, RANKL is an essential factor for osteoclastogenesis [26,27], and upregulation leads to abnormal bone resorption. Therefore, we chose to examine MMP-3, ADAMTS-4, and RANKL as joint-damage-related molecules. In this study, we measured mRNA expression of these molecules, rather than the proteins themselves, because large amounts of these proteins are already present in RA-SF.
The addition of RA-SF to the incubation medium induced MMP-3 and RANKL mRNA expression in RA-FLS, and induced MMP-3 and ADAMTS-4 mRNA expression in chondrocytes. Although a variety of cytokines exist in RA-SF, we focused on IL-1β, IL-6, and TNF-α because their inhibitors are widely used in the treatment of RA patients. As shown in Table 1, IL-6, TNF-α, and IL-1β (in part) are detectable in RA-SF. All cytokine inhibitors showed significant inhibitory effect on RA-SF-induced MMP-3, ADAMTS-4, and RANKL mRNA expression, but none achieved complete inhibition even if the concentration of inhibitors was increased. These results suggest that many cytokines play a role in the mRNA expression of MMP-3, ADAMTS-4, and RANKL.
| Sample ID | CRP (mg/L) | Other disease | Treatment | IL-6 (ng/mL) | sIL-6R (ng/mL) | TNF-α (pg/mL) | IL-1β (pg/mL) |
|---|---|---|---|---|---|---|---|
| 1 | 15 | Chronic cystitis | Diclofenac | 2.1 | 14.4 | 66.0 | Not detected |
| 2 | 32 | Prostatitis, urolithiasis | Nimesulide | 55.9 | 14.7 | 56.0 | 377.8 |
| 3 | 16 | None | Nimesulide | 89.3 | 10.4 | 45.4 | 176.4 |
| 4 | 12 | None | Leflunomide, diclofenac | 1.0 | 12.3 | 45.4 | Not detected |
| 5 | 17 | Chronic gastritis, osteochondrosis | Leflunomide, nimesulide, methylprednisolone | 4.8 | 16.5 | 71.0 | Not detected |
Table 1: Characteristics of the synovial fluids from five RA patients.
We also showed that HA suppressed RA-SF-induced MMP-3, ADAMTS-4, and RANKL expression in RA-FLS and chondrocytes. These are reasonable results, because we and others have reported that HA inhibits IL-1β- or IL-6-induced production of MMP and ADAMTS in RA-FLS and chondrocytes [15,16]. Although the inhibitory mechanism of HA is not fully understood, it is reported that the binding of HA to CD44 or ICAM-1 is essential for the induction of the inhibitory effect [28,29], and we and others have shown that HA induces MKP-1, a negative regulator of MAPK, and IRAK-M, a negative regulator of toll-like receptor signaling, and inhibited cytokine induced signal transductions [15,16].
HA is a major component of synovial fluid and cartilage matrix, and it is responsible for the viscoelastic qualities of synovial fluid, acting as both a lubricant and shock absorber. However, in joints affected by OA and RA, high-molecular-weight HA is cleaved into low-molecularweight HA which has low viscoelasticity [13]. Therefore, intra-articular injection of HA makes up for the loss of viscoelasticity of synovial fluid and protects against degradation of cartilage.
Each cytokine inhibitor partially suppressed RA-SF-induced expression of MMP-3, ADAMTS-4, and RANKL. These results lead to the idea that a combination of cytokine inhibitors might more potently inhibit the expression of these molecules. However, therapy with a combination of cytokine inhibitors is not recommended because of the strong immune-suppressing effect and high cost. HA on the other hand is very safe and low-cost, and is approved in Japan for therapy to reduce knee-joint pain in RA patients; therefore, we examined the combination effect of HA and a cytokine inhibitor.
To improve the quality of life of RA patients it is important to prevent joint destruction. Seki et al. [12] indicated the possibility that large joints are more resistant to the effects of cytokine inhibitors than are small joints. Reasons for this may be that larger amounts of drug are necessary to suppress joint destruction in large joints than are necessary in small joints or that weight bearing prevents the beneficial effects of the cytokine inhibitor. We demonstrated here that the combination of HA and a cytokine inhibitor more potently suppressed the expression of MMP-3, ADAMT-4, and RANKL than did cytokine inhibitor alone.
In conclusion, the combination of HA and cytokine inhibitor may be beneficial for the therapy of large joints of RA patients because the combination more effectively suppresses the expression of joint-damage- related molecules and HA makes up for the lost viscoelasticity of the synovial fluid.
