Research Article - (2015) Volume 4, Issue 3
Rheumatoid (RA) and Psoriatic arthritis (PsA) are characterized by extensive synovitis resulting in bone destruction in both diseases and new bone formation in PsA. Objective: This prospective study analyzed interleukin (IL)-6, IL-17, IL-23, tumor necrosis factor (TNF)-α serum and synovial fluid (SF) levels and osteoprotegerin (OPG), bone-specific alkaline phosphatase (BAP) and D-vitamin (D-Vit) serum levels in RA and PsA patients before and after anti-TNF-α. Methods: 15 RA and 15 PsA patients with knee effusion and starting adalimumab (ADA) treatment were enrolled. Serum and SF from inflamed knee joint samples were obtained at baseline and after 24 weeks of treatment. Statistical analysis was performed using Graph Pad 5.0 statistical software. Results: In RA and PsA, SF IL-6, IL-17, and TNF-α were higher than serum levels while higher serum IL-23 was detected than in SF. Higher serum/SF IL-6, IL-23 and SF TNF-α were observed in RA than PsA, while serum IL-17 was higher in PsA than RA. Positive feedback among IL-6, IL-23, IL-17 and CRP and negative correlation between IL-17 and TNF-α in RA were found. In PsA, IL-23 correlated positively with IL-6. OPG correlated positively with ESR/CRP in RA and PsA. D-Vit correlated negatively with OPG and ESR in PsA. Higher BAP in RA than PsA and positive correlation with IL-6 in RA and with OPG in PsA were noticed. In PsA, IL-6 and OPG serum levels decreased significantly after 24 weeks ADA treatment. Conclusions: Distinct distribution of inflammatory cytokines and correlations with bone mediators were detected in RA and PsA. ADA affected inflammatory cytokines and bone mediators in PsA patients.
Keywords: Synovial fluid; Inflammatory arthritis; Anti-TNF-α; Inflammatory cytokines; Bone mediators; D-vitamin
RA: Rheumatoid Arthritis; PsA: Psoriatic Arthritis; TNF-α: Tumor Necrosis Factor -alpha; RANKL: Receptor Activator of Nuclear Factor Kappa-B Ligand; OPG: Osteoprotegerin; FLS: Synovial Fibroblasts; SpA: Spondyloarthitis; BAP: Bone-Specific Alkaline Phosphatase; D-Vit: D-vitamin; ADA: Adalimumab; VAS: Visual Analogue Scales; DAS44-ESR: Disease Activity Score 44-Erythrocyte Sedimentation Rate; PASI: Psoriasis Area and Severity Index; EULAR: European League Against Rheumatism; DMARDs: Disease Modifying Anti-rheumatic Drugs; SF: Synovial Fluid; ESR: Erythrocyte Sedimentation Rate; CRP: C-reactive Protein; ELISA: Enzyme-Linked Immuno Sorbent Assay
Rheumatoid arthritis (RA) and Psoriatic arthritis (PsA) are chronic inflammatory joint diseases that share some features such as the extensive synovitis resulting in erosions of articular cartilage leading to bone destruction and radiological damage [1,2]. Osteoimmunology is an expanding field demonstrating that bone is a dynamic organ interacting with the immune system [3]. A wide range of molecular and cellular interactions between bone and immune system have been demonstrated especially in RA, while less evidence exists in PsA [4,5]. Interleukin (IL)-17 producing T helper (h) cells are critical in the pathogenesis of both RA [6] and PsA [7]. IL-17 has been detected at high levels in the serum, synovial fluid (SF), and synovium of these patients [8]. This cytokine enhances local inflammation by increasing the production of IL-1, IL-6, IL-8, and tumour necrosis factor-α (TNF-α), the last one promotes the expression and the activity of the receptor activator nuclear factor kappa-B ligand (RANKL) [9,10]. Furthermore, IL-17 directly induces osteoclastogenesis up-regulating RANKL on mesenchymal cells, such as osteoblasts and synovial fibroblasts (FLS) [11]. RANKL also acts on mature osteoclasts and activates the boneresorbing activity and survival of these cells [12,13]. The other important actor in this system is osteoprotegerin (OPG), a soluble receptor of RANKL belonging to the TNF receptor superfamily. OPG specifically binds to RANKL and inhibits its activity by preventing the binding to RANK with the inhibition of bone erosions [14]. Furthermore, Th17 cells express higher levels of RANKL than Th1 and Th2 cells [15]. Th17 cells represent an osteoclastogenic T cell subset and a link between the abnormal T cell response and bone damage [16-18]. Moreover, SF of PsA patients is enriched with Th17 cells and IL-17 receptor expression is higher in FLS form RA and PsA patients in comparison to FLS from osteoarthritis patients [19,20]. IL-23 is a member of the IL-12 cytokine family. It is up-regulated in RA FLS and its expression is positively controlled by the presence of IL-17A. IL-23 induces also Th17 cell differentiation and IL-17A production. Thus, a positive feedback loop between IL-23 and IL-17A may drive synovial inflammation in RA and PsA [21,22]. TNF-α-blocking agents cause a deep and sustained inhibition of bone erosion in RA and PsA patients [23,24]. However, it is unknown whether these agents also affect bone and enthesophyte formation typically observed in PsA [24]. Vitamin D (D-Vit) is a crucial actor in the interplay between immune system and bone tissue. Active metabolite of D-Vit (1,25OH2D3) inhibits the synthesis of IL-1, IL-6, IL-12 and TNF-α by macrophages and low D-Vit levels may increase the development of self-reactive T cells [25,26]. Moreover, data from literature suggested an inverse association between disease activity and serum D-Vit levels in RA and Psoriasis [27,28].
The aim of this study was to assess serum and SF levels of inflammatory cytokines as IL-6, IL-23, IL-17, TNF-α and bone metabolism mediators D-Vit, OPG, bone-specific alkaline phosphatase (BAP) in RA and PsA patients at baseline and after anti-TNF-α treatment.
Patients
We enrolled consecutive RA (n=15) and PsA (n=15) patients presenting a knee joint effusion that were classified according to the American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) classification criteria for RA and the Classification criteria for psoriatic arthritis (CASPAR criteria) for PsA [29,30]. Both RA and PsA patients had an active disease (according with disease activity score, DAS44), inadequate response to standard disease-modifying anti-rheumatic drugs (DMARDs), and were not previously treated with anti-TNF-α drugs. All the patients commenced adalimumab (ADA) (40 mg every other week subcutaneously). Demographic and clinical features of patients are shown in Table 1.
| RA (n= 15) | PsA (n= 15) | P value | |
|---|---|---|---|
| Sex (M/F) | 4/11 | 7/8 | Ns |
| Age (year) | 56.7 ± 13.5 | 53.4 ±11.9 | Ns |
| Disease duration (months) | 15.1±18.7 | 14.7±16.4 | Ns |
| ESR (mm/h) | 27 ± 26.9 | 39.9 ± 24.2 | Ns |
| CRP (mg/L) | 12.3 ± 15.6 | 6.2 ± 11.5 | Ns |
| DAS | 5.8 ± 0.8 | 5.5 ± 1.1 | Ns |
| PASI | NA | 4.3±3.2 | |
| RF (n/%) | 10/66.6 | 0/0 | 0.0002 |
| ACPA (n/%) | 11/73.3 | 0/0 | <0.0001 |
| NSAIDs (n/%) | 2 (13.3) | 3 (20) | |
| Prednisone <7.5 mg/day (n/%) | 10 (66.6) | 6 (40) | |
| DMARDs (n/%) | 8 (53.3) | 6 (40) |
Data are expressed as mean ± standard deviation, unless differently specified. Statistical comparisons were performed by Student’s t-test or Fisher’s exact test as appropriate. RA, rheumatoid arthritis; PsA, psoriatic arthritis; NA, not applicable; Ns, not significant; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; DAS, disease activity score; PASI, psoriasis area and severity index; RF, rheumatoid factor, ACPA, anti-citrullinated protein/peptide antibodies; NSAIDs, non-steroidal anti-inflammatory drugs; DMARDs, disease-modifying anti-rheumatic drugs.
Table 1: Demographic, clinical, and laboratory data of Rheumatoid Arthritis and Psoriatic Arthritis patients.
We collected blood samples from all patients at baseline and after 24 weeks since the beginning of ADA treatment. The sera, together with paired SF, obtained at baseline by therapeutic arthrocentesis, were stored at -80°C until levels of cytokines and bone metabolism mediators were measured.
Patients affected by osteoporosis were excluded as well as patients treated with bisphosphonates, oral calcium/D-Vit.
All the patients of this study were prospectively enrolled from the rheumatology outpatient clinic at University of Rome “Tor Vergata”, Italy. At recruitment (T0) and after 24 weeks (T24) of ADA treatment, clinical assessment included tender and swollen joint count for DAS (44 joint count for swelling, 4 variables, and erythrocyte sedimentation rate-based) calculation [31], while laboratory assessment included erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP). The treatment was fully in compliance with the Helsinki declaration and all study subjects provided their informed consent.
Laboratory analysis
Serum samples were obtained at T0 and at T24 and were stored at -80°C until analyzed. Paired SF was obtained from the inflamed knee joint at T0. ESR was determined with the Westergren method. Serum CRP was measured by nephelometry with an automatic analyser according to the manufacturer’s instructions. Calcium and parathormone (PTH) levels were determined prior to treatment to exclude metabolic bone diseases. Commercially available human ELISA kits were employed to determine IL-6, IL-23, IL-17, TNF-α (Quantikine, R&D Systems, Minneapolis, MN), OPG levels (Biomedica Medizinprodukte, GmbH &Co, Austria) and BAP (QUIDEL, San Diego, CA, USA), following the manufacturer’s instructions. Serum total 25(OH)D3 levels were measured by radioimmunoassay (DiaSorin, Stillwater, MN). D-Vit deficiency was defined as serum 25(OH)D3 levels <30 ng/ml.
Statistical analysis
To test normality of data sets the D’Agostino and Pearson omnibus test was used. Normally distributed variables were summarized using mean ± standard deviation. To test if the means of two samples were different the Student’s t-test was used for normal distributed data sets. We applied the one-way ANOVA with Bonferroni correction for multiple testing. Data in the longitudinal analysis during the treatment course of individual patients were evaluated with the nonparametric Wilcoxon signed-rank test. Univariate comparisons between nominal variables were performed by Fisher’s exact test. The significance of any correlation was determined by Pearson’s correlation coefficient for normal variables. P values <0.05 were considered significant. The statistical analysis was performed using Graph Pad 5.0 statistical software (GraphPad Prism, San Diego, CA, USA).
Serum and SF concentrations of IL-6, IL-23, IL-17 and TNF-α were measured in 15 RA patients and 15 PsA patients. Bone turnover mediators D-Vit, OPG and BAP levels were evaluated in sera of the same RA and PsA patients. Serum levels of these inflammatory cytokines and bone turnover mediators were also assessed after 24 weeks of ADA treatment.
Cytokines and bone turnover mediators in serum and synovial fluid of RA and PsA patients
No significant differences were observed in sex, age, disease duration and DAS between RA and PsA patients (Table 1).
IL-6, IL-23, IL-17 and TNF-α levels were measured in paired sera and SF from 15 RA patients and 15 PsA patients (Table 2).
| RA T0 | RA T24 | P value | PsA T0 | PsA T24 | P value | ||
|---|---|---|---|---|---|---|---|
| ESR (mm/h) | 27 ± 26.9 | 17.3 ± 17 | 0.008 | 39.9 ± 24.2 | 16.9 ± 0.6 | 0.0006 | |
| CRP (mg/dl) | 12.3 ± 15.6 | 5.1 ± 7.1 | 0.004 | 6.2 ± 11.5 | 0.2 ± 0.3 | 0.0002 | |
| DAS | 5.8 ± 0.8 | 3.7 ± 1.4 | 0.0001 | 5.5 ± 1.1 | 2 ± 0.8 | 0.0001 | |
| IL-6 (pg/ml) | Serum SF | 171.2 ± 254.2 14153 ± 4646 | 421.1 ± 552.8 NA | ns | 32.7 ± 16.2 757.9 ± 170.7 | 23.7 ± 8.7 NA | 0.04 |
| IL-23 (pg/ml) | Serum SF | 807.6 ± 804.7 53.1 ± 27.1 | 1226.1 ± 1544.9 NA | ns | 156.3 ± 216.7 24.4 ± 4 | 181.8 ± 147.7 NA | ns |
| IL-17 (pg/ml) | Serum SF | 7.1 ± 0.3 21.7 ± 8.1 | 7.9 ± 1.1 NA | ns | 8.1 ± 1.8 24 ± 7.7 | 7.9 ± 1.4 NA | ns |
| TNF-α (pg/ml) | Serum SF | 20.8 ± 19.4 354.4 ± 84.5 | 74.9 ± 63.4 NA | 0.0005 | 27.5 ± 51.5 252.6 ± 56.9 | 47.7 ± 28.6 NA | 0.08 |
| D-vit (ng/ml) | Serum | 28.3 ± 9.3 | 35 ± 8.7 | ns | 23.4 ± 10.2 | 36.6 ± 8.1 | ns |
| BAP (U/L) | Serum | 16.8 ± 6.8 | 18.7 ± 9.2 | ns | 10.9 ± 4.2 | 9.2 ± 2.1 | ns |
| OPG (pg/ml) | Serum | 3.7 ± 1.2 | 4.1 ± 2.1 | ns | 3.5 ± 1.3 | 2 ± 0.7 | 0.04 |
Data are expressed as mean ± standard deviation. Statistical comparisons were performed by Wilcoxon signed-rank test. RA, rheumatoid arthritis; PsA, psoriatic arthritis;
NA, not applicable; Ns, not significant; ESR, erythrocyte sedimentation rate; CRP, C-reactive protein; IL, interleukin; TNF-α, tumor necrosis factor-α; DAS, disease activity
score; SF, synovial fluid; D-Vit, Vitamin D; BAP, bone-specific alkaline phosphatase; OPG, osteoprotegerin.
Table 2: Disease activity scores and levels of cytokines/bone mediators in Rheumatoid Arthritis and Psoriatic Arthritis patients at baseline and after 24 weeks of Adalimumab
In RA patients levels of IL-6 (p<0.0001), IL-17 (p<0.0001) and TNF-α (p<0.0001), were higher in SF than those in sera. On the contrary, levels of IL-23 were higher in serum than those in SF (p=0.005) (Figure 1A-D). Similarly in PsA patients, levels of IL-6 (p<0.0001), IL-17 (p<0.0001) and TNF-α (p<0.0001) were higher in SF than those in sera while IL-23 levels were higher in serum than those in SF (p=0.007) (Figure 1A-D).
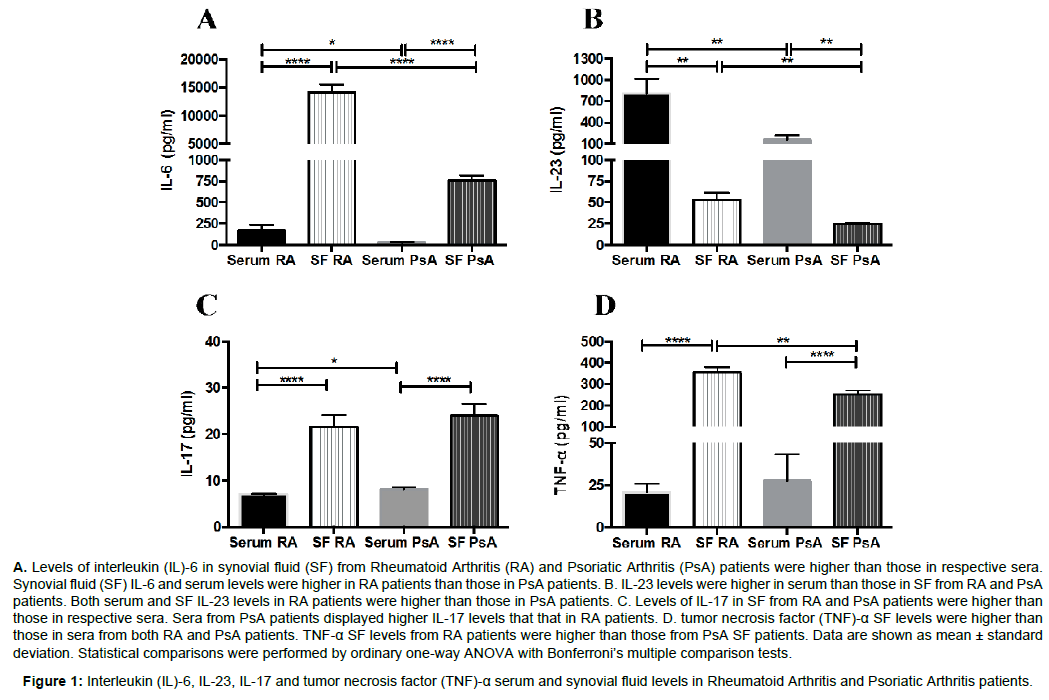
Figure 1: Interleukin (IL)-6, IL-23, IL-17 and tumor necrosis factor (TNF)-a serum and synovial fluid levels in Rheumatoid Arthritis and Psoriatic Arthritis patients.
We also compared levels of these cytokines between RA and PsA patients. Both serum and SF levels of IL-6 were significantly higher in RA patients than those in PsA patients (p=0.04 and p<0.0001, respectively). Likewise, serum and SF IL-23 levels were higher in RA patients than those in PsA patients (p=0.006 and p=0.008, respectively). On the contrary, IL-17 serum levels resulted significantly higher in PsA patients than those in RA patients (p=0.04). IL-17 SF levels and TNF-α serum levels were similar in RA and PsA patients. SF concentration of TNF-α was significantly higher in RA patients than that in PsA patients (p=0.009) (Figure 1A-D).
In RA patients, a positive correlation was observed between IL-23 serum levels and both IL-6 serum levels and CRP values (p<0.0001 and p=0.02, respectively). Moreover, a positive correlation was demonstrated between IL-17 SF levels and both IL-6 and IL-23 serum levels (p=0.001 for both comparisons). IL-17 SF levels correlated positively also with CRP values (p=0.04), while TNF-α SF levels correlated with IL-23 SF levels (p=0.01). A negative correlation was found between IL-17 serum levels and TNF-α serum levels (p=0.01) (Figure 2A-G). In PsA patients a positive correlation was observed between IL-23 serum levels and both serum/SF IL-6 levels (p=0.02 and p=0.03, respectively) (Figure 3A and 3B). No other significant correlation was found between serum/ SF cytokines levels and ESR, CRP, DAS in both RA and PsA patients.
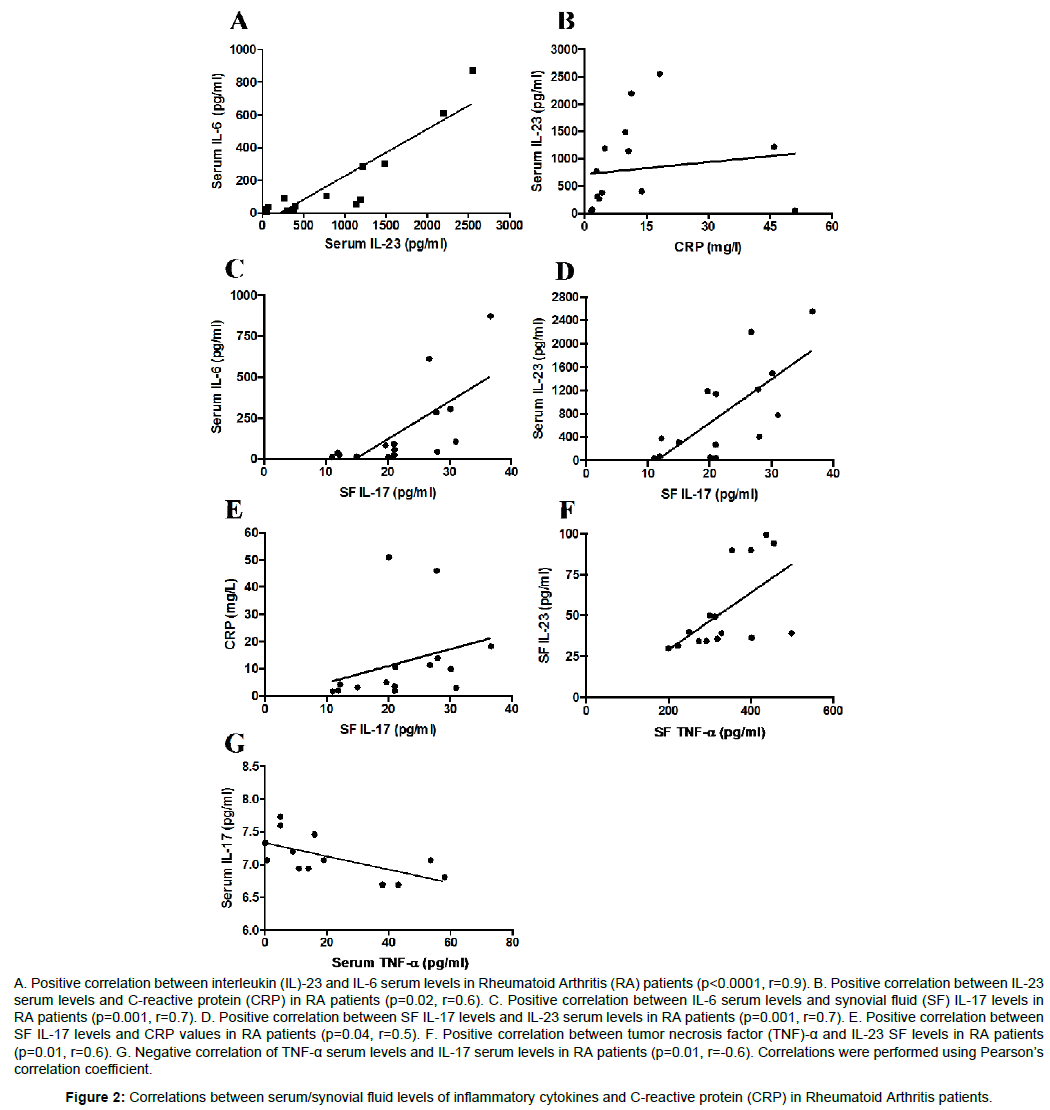
Figure 2: Correlations between serum/synovial fluid levels of inflammatory cytokines and C-reactive protein (CRP) in Rheumatoid Arthritis patients.
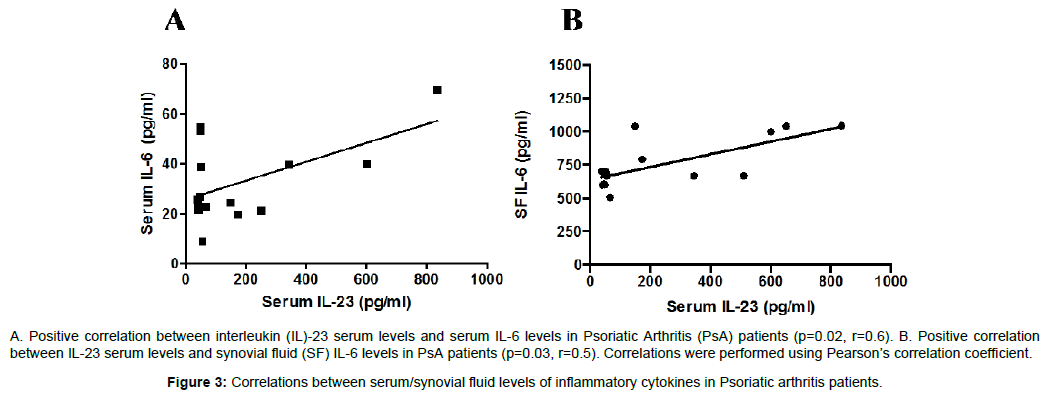
Figure 3: Correlations between serum/synovial fluid levels of inflammatory cytokines in Psoriatic arthritis patients.
Bone turnover mediators D-Vit, OPG and BAP levels were evaluated in sera of the same RA and PsA patients (Table 2). Calcium and PTH levels were also measured and resulted within normal ranges in these patients (data not shown).
D-Vit and OPG serum levels were similar in the two groups of patients. However, baseline serum levels of D-Vit were low in respect to normal range both in RA and PsA patients (Table 2), noted as D-Vit deficiency. BAP serum levels in RA patients were higher than those in PsA patients (p=0.009) (Figure 4A). In both RA and PsA patients, the mean levels were significantly higher compared with normal range (data not shown). In RA patients a positive correlation was observed between BAP and SF IL-6 levels (p=0.01). Moreover, a positive correlation was demonstrated between OPG and ESR levels (p=0.04) (Figure 4B-C). In PsA patients a positive correlation was observed between OPG and both ESR and CRP levels (p=0.001 and p=0.004, respectively). On the contrary, D-Vit serum levels correlated inversely with both ESR and OPG levels (p=0.04 for both comparisons) (Figure 5A-E). No other significant correlation was observed between serum bone mediators and ESR, CRP, DAS both in RA and PsA patients.
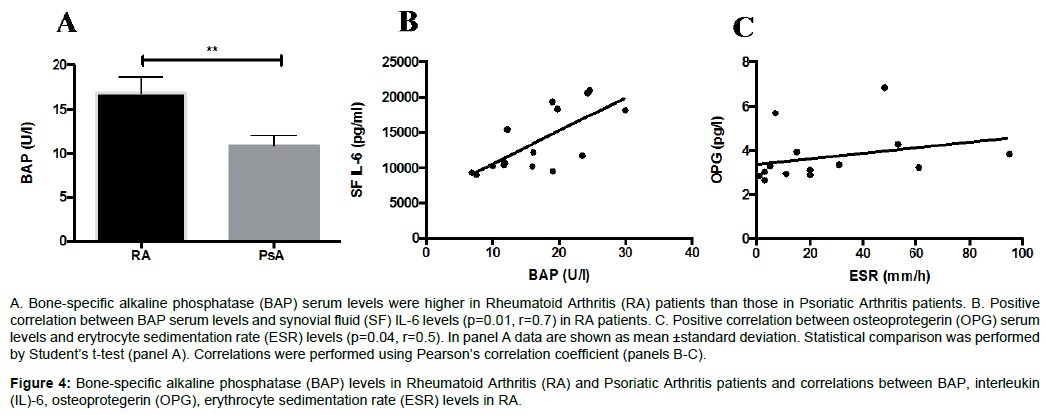
Figure 4: Bone-specific alkaline phosphatase (BAP) levels in Rheumatoid Arthritis (RA) and Psoriatic Arthritis patients and correlations between BAP, interleukin (IL)-6, osteoprotegerin (OPG), erythrocyte sedimentation rate (ESR) levels in RA.
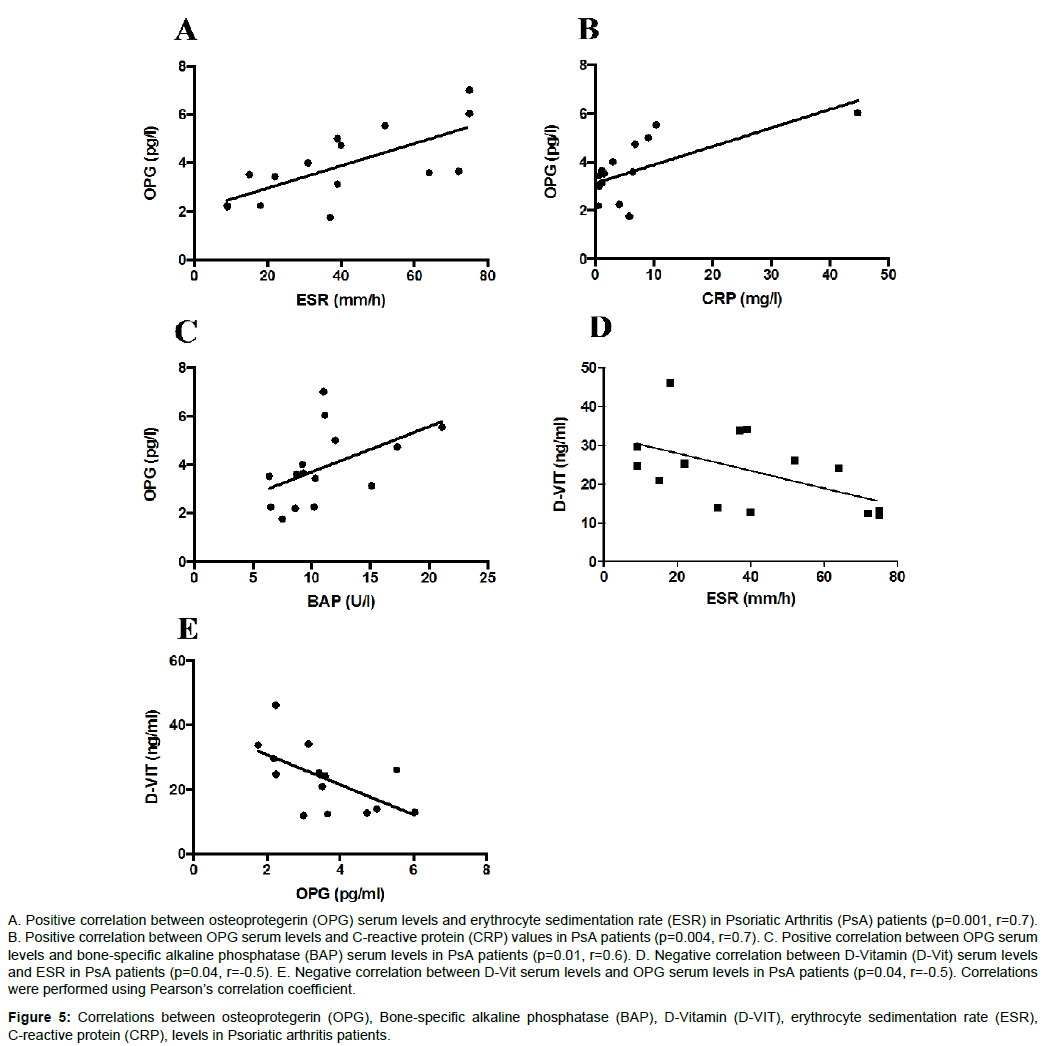
Figure 5: Correlations between osteoprotegerin (OPG), Bone-specific alkaline phosphatase (BAP), D-Vitamin (D-VIT), erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), levels in Psoriatic arthritis patients.
Effect of ADA treatment on IL-6, IL-23, IL-17, TNF-α, D-Vit, OPG and BAP serum levels in RA and PsA patients
All patients were naïve for biologic therapy at baseline and started with ADA. Serum levels of inflammatory cytokines IL-6, IL-23, IL- 17, TNF-α, and bone turnover mediators D-Vit, OPG and BAP were measured in RA and PsA patients at baseline (T0) and after 24 weeks of ADA treatment T(24). Data are shown in Table 2.
In RA patients an increase of TNF-α serum levels was observed at T24 compared with T0 (p=0.0005).
In PsA patients a reduction of IL-6 and OPG serum levels was observed at T24 compared with T0 (p=0.04 for both comparison).
No other significant modification in serum levels of cytokines and bone turnover mediators were detected in both RA and PsA patients. Both RA and PsA patients showed a significant reduction of DAS levels after 24 weeks of ADA treatment (p=0.0001 for both comparisons).
Previous studies demonstrated several differences between RA and PsA pathogenesis although they share some important features such as target molecules of biologic treatments. This study has reported a distinct distribution of inflammatory cytokines with IL-6, IL-17 and TNF-α prevalently localised in SF, while IL-23 in serum of both RA and PsA patients. Moreover, a different pattern of cytokine detection was found between RA and PsA: high serum/SF IL-6 and IL-23 and SF TNF-α level in RA, while serum IL-17 was higher in PsA than RA patients. We can speculate that the prevalent detection of IL- 23 in serum from both RA and PsA patients mirrors the systemic inflammatory response as demonstrated by its correlation with CRP levels in RA. On the contrary, higher SF levels of IL-6, IL-17 and TNF-α support the hypothesis of their major contribution locally, in joint inflammation, at the target tissue [32,33]. Statistically significant higher serum levels of IL-17 were observed in PsA than in RA, probably due to the elevated frequencies of IL-17 and IL-22 producing CD4+ T cells in PsA [34]. TNF-α levels didn’t discriminate between the two diseases, because of its common role in the pathogenesis of RA and PsA. These results highlight how the IL-23/IL-17 axis could be considered a major pro-inflammatory pathway, both systemic and local, in chronic inflammatory diseases as RA and PsA [35]. Furthermore, the indirect correlation between IL-17 and TNF-α sera level might support the independent role of IL-17 from TNF-α in RA pathogenesis. Several positive correlations among cytokines and inflammatory markers both in RA and PsA arose from this study. Correlations among IL- 6, IL-23, IL-17 and TNF-α level demonstrated a positive feedback in the inflammatory cascade in RA. In accordance with data from literature, higher levels of BAP were noticed in both RA and PsA patients compared with healthy controls, pointing out its involvement in periarticular bone changes [36,37]. In this context, correlation with SF IL-6 levels was shown supporting the local production of BAP in RA joints previously reported, suggesting that local BAP production might occur in the arthritic joints [38]. Furthermore, in PsA BAP was positively correlated with OPG levels. OPG is a relevant bone anabolic marker strongly associated with inflammatory markers in both diseases. In accordance with these results PsA patient had significant reduction of OPG levels after ADA treatment, whereas this was not observed in RA patients. This result is in line with a prospective study performed by Ramonda et al. [39] who showed that anti-TNF-α treatment had a negative effect on OPG concentration [39]. This could be considered a suitable serum biomarker of response to ADA treatment in PsA patients. Recently, it has been demonstrated that D-Vit can inhibit the synthesis of mRNA of macrophages-derived cytokines such as IL-1, IL- 6, IL-12 and TNF-α [32]. In fact, D-Vit is actually considered as an immunomodulatory mediator; in our study both RA and PsA patients showed D-Vit deficiency and, in agreement with Braun-Moscovici et al., no correlation was demonstrated between D-Vit levels and disease activity score in our cohorts [40]. However, in PsA patients D-Vit levels showed a negative correlation with ESR and OPG levels. Anti-TNF-α treatment may affect cytokines and cells in both RA and PsA patients [41,42]. In line with the inflammatory nature of IL-6, serum IL-6 levels in PsA patients are decreased after ADA treatment. This reduction was associated with a decrease in ESR, CRP and DAS levels suggesting a role of IL-6 as a valuable inflammatory biomarker in PsA. Changes in IL-23 and IL-17 levels after TNF-α blockade were not observed in our patient cohort treated with ADA suggesting that they are not influenced by anti-TNF-α. In this study, levels of TNF-α were increased after 24 weeks of ADA treatment in RA patients and a trend was observed also in PsA patients. This increase could be explained by an inhibition of synovial inflammation by the drug and marginalization of TNF-α in the blood after 24 weeks of ADA treatment. This could explain the relapse of the disease when treatment is interrupted [43]. The action of TNF-α and other inflammatory cytokines is not limited to local inflammation but it involves directly and indirectly the activation of osteoclasts [44]. The effect of anti-TNF-α on bone mineral density (BMD) in RA and SpA patients has been extensively examined but studies that specifically examine cytokines and bone turnover in RA and PsA patients are lacking. Several studies in patients with RA and Spondyloarthritis demonstrated an increase of BMD after treatment with TNF-α inhibitors [45-47]. Some authors showed a possible effect of anti-TNF-α on Th17/T regulatory imbalance, which could partially explain the anti-resorptive effect of these agents, because of the pivotal role of Th17 and IL-17 in pathogenesis of bone damage [34]. In our PsA treated patients, a significant reduction of OPG levels was demonstrated consistent with the fact of an inhibition of radiographic progression by ADA.
Conversely rising levels of circulating Th17-cells and IL-17 were observed in patients with an inadequate response to anti-TNF-α therapy [35]. However, these finding were not observed in our study cohort since all the patients enrolled showed a good clinical response during ADA treatment. This study has some limits, such as the low number of patients enrolled, the lack of both radiographic score evaluation (due to the short follow-up) and SF samples after the treatment.
In summary, this study evaluated the relationship between the local and systemic expression of key mediators of inflammation and their association with bone metabolism both in RA and PsA patients. This study describes a different distribution of inflammatory cytokines between serum and SF in RA/PsA and their modification during anti- TNF-α treatment. Moreover, the regulation of the Th17 cytokine system and bone metabolism mediators resulted different between RA and PsA.
MSC and PC equally contributed to the paper and have written the manuscript. MM, RZ, LN, PT and CP have performed the human sample collection, elaborated the scientific primary data, handled and contributed to the first draft of the manuscript. SB has elaborated the scientific results. RP conceived the project and supervised the study.
