Research Article - (2015) Volume 0, Issue 0
Objective: Inflammatory back pain (IBP) in Ankylosing Spondylitis (AS) and Undifferentiated Spondyloarthritis (UspA) adversely affects the quality of life. Herein combination DMARD vs. sulfasalazine (SSZ) monotherapy was evaluated in treatment of axial symptoms of AS and UspA.
Methods: Patients with AS/UspA with disease duration ≤ 8 years, IBP of atleast 6 months duration, and BASDAI ≥ 4 or early morning stiffness ≥ 1 hour despite NSAID therapy for 6 weeks were included. Patients were initiated on SSZ with either combination DMARD [MTX (10 mg escalated by 2.5 mg every week up to 20 mg/week) and HCQS 200 mg/day] or SSZ Monotherapy group [placebo MTX and placebo HCQS]. ASAS20 response was assessed at baseline and at the end of 6 months.
Results: Of thirty three patients (31 males) with mean disease duration 39 months and mean BASDAI of 6 at baseline, 27 completed the study (16 in Combination DMARD and 11 in SSZ monotherapy group). ASAS 20 response, was achieved in 68.4% (13/19) and 50% (7/14) in the Combination DMARD and SSZ monotherapy groups (p=0.47), respectively. BASDAI scores decreased significantly in both the groups after therapy. A significant improvement in BASFI, patient pain VAS, patient global disease VAS, HAQ, and MCS of SF-36 was observed in both the groups. In the combination DMARD group, significant improvement in BASMI, FACIT and PCS of SF-36 and decrease in the serum MMP-3 levels was observed following therapy.
Conclusion: SSZ monotherapy is equally efficacious as combination DMARD group in a significant proportion of patients with NSAID refractory IBP associated with AS/ USpA.
Keywords: Inflammatory back pain; Spondyloarthritis; Ankylosing spondylitis; Psoriatic arthritis; Reactive arthritis; Inflammatory bowel disease
Seronegative Spondyloarthropathies (SpA) refer to a group of chronic inflammatory disorders of unknown etiology. With prevalence between 0.5-2.5 percent, they are among the most common rheumatologic disorders [1]. This is a male predominant disease with a mean age of onset usually in the second and third decade. This includes a heterogeneous group of patients with predominant axial skeletal and entheseal involvement to more wide spread peripheral involvement; asymmetric or symmetric oligo/polyarthritis without any axial involvement. The subgroups which come under this terminology includes: Ankylosing Spondylitis (AS), Psoriatic Arthritis, Reactive Arthritis, Inflammatory bowel disease associated arthritis and Undifferentiated Spondyloarthritis (USpA).
These diseases are major cause of morbidity for the patients, causing pain, stiffness, loss of mobility, disability, poor sleep and overall poor quality of life. In a study conducted by Linden et al., it was found that work related indices such as percentage of unemployment, lack of permanence of work, number of sick leaves and early retirement due to illness were all higher in patients with AS as compared to healthy individuals [2]. In another study, it was demonstrated that the quality of life in these patients is worse than cancer and myocardial infarction patients [3]. Amor et al., concluded that predictive factors of long term outcome could be defined very early after the onset of spondyloarthropathy [4]. It has been demonstrated that a major factor which influences the quality of life is the extent of entheseal involvement and associated stiffness and pain [5]. Besides these, the economic impact of loss of productivity due to AS calculated in terms of average annual human capital lost varies from Euros 4227 to Euros 8862 per patient.
NSAIDS have been the main stay of treatment for these diseases for long. Despite providing good pain relief, they are largely ineffective in altering the natural course. However, very often, in spite of therapy, pain and discomfort continues in these patients with recurrent exacerbations.
The DMARDs (Disease Modifying Anti Rheumatic Drugs) are a group of drugs which have come into prominence following their remarkable efficacy in the management of rheumatoid arthritis. The major drugs representative of this group are; methotrexate (MTX), sulfasalazine (SSZ), hydroxychloroquine (HCQ), gold and leflunomide. Of these drugs, the most well studied drug in SpA is SSZ. However, its efficacy has been variably reported. Dougdas et al., conducted a multicenter, 36 week trial, involving 264 patients with evidence of active AS refractory to NSAIDs, defined as morning stiffness of >45 minutes duration, inflammatory back pain, and patient and physician global assessments of moderate or high disease activity. The primary outcome variable was treatment response based on morning stiffness, back pain, and physician and patient global assessments. In this trial, SSZ was given at a dose of 2 g/day. The trial found SSZ to be no more effective than placebo; treatment response rates were 38.2% for SSZ versus 36.1% for placebo. Significant treatment efficacy was not shown for any of the following four outcome measures used to define treatment response: physician global assessment (SSZ, 53.4% vs. placebo, 55.6%) patient global assessment (SSZ, 40.5% vs. placebo, 42.1%) morning stiffness (SSZ, 48.9% vs. placebo,44.4%) and back pain (SSZ, 23.7% vs. placebo, 27.1%). Premature discontinuation rates due to adverse events were 8% (11/131) and 5% (6/133) for SSZ and placebo, respectively [6]. A major reanalysis of a series of randomized, double blind, placebo controlled, 36 week multicenter trials of SSZ (2 g/day) (including the above study) on the axial and peripheral articular manifestations of AS (n=264), psoriatic arthritis (n=221), and reactive arthritis (n=134) was recently reported of which 187 patients had only axial manifestations, while 432 patients had peripheral arthritis. The primary outcome measure was treatment response, determined on the basis of improvement in four outcome measures: patient and physician global assessments (all patients), morning stiffness and back pain in patients with axial manifestations, and joint pain/tenderness scores and joint swelling scores in patients with peripheral articular manifestations. Intention to treat analysis showed that SSZ provided significant improvement in patients with peripheral arthritis; response rates were 59.0% in patients treated with SSZ versus 42.7% in the placebo group (p=0.0007). They did not find SSZ to be beneficial for axial or entheseal disease [7]. However Braun et al. had demonstrated the efficacy of SSZ in inflammatory backache due to USpA and early AS, in patients without peripheral arthritis [8].
The other major DMARD tried in AS is methotrexate (MTX). Though MTX monotherapy has not been found to be effective in axial symptoms of SpA in a number of studies, it has been reported to be useful in patients with peripheral arthritis [9-13]. Gonzalez-Lopez et al., reported significant improvement with MTX in physical well-being, BASDAI, BASFI, physician and patient global assessments, the HAQ, and spinal pain [14]. Haibel et al. studied the role of subcutaneous MTX at doses of 20 mg/week for 16 weeks in a NSAID refractory AS patients with axial symptoms and found ASAS 20, 50 and 70 responses of 25%, 10% and none respectively, with no change in BASDAI [11]. In a recent Cochrane review, it was concluded that MTX may not improve overall disease activity, physical function, overall pain, tenderness or swelling in the ligaments of the joints, movement of the spine, stiffness and overall well-being [15].
Leflunomide, the other major DMARD, has also fared poorly in a controlled trial in ankylosing spondylitis [16]. At present, there is inadequate data regarding the efficacy of HCQ for inflammatory backache. Apart from SSZ, there is no data available on the utility of DMARDS in USpA.
The discovery of anti-TNF-α based biologics have been the major breakthrough in the management of SpA in recent times [17]. These drugs, besides providing symptomatic improvement, also improve disease activity indices. However, as of now, they have not demonstrated a definite benefit in halting radiologic progression [18]. Besides, the enormous cost incurred at a rate of about Rs 700,000/- (Euros 10000, US $ 14000/-) per annum, put it out of reach of the majority of affected population in India and other third world nations. Added to these, is the increased risk of tuberculosis and fungal infections, a major problem in our country.
In this background, there is a severe and pressing need for alternative safe and effective drugs in the management of these diseases. It is here that the combination DMARD therapy assumes importance as a potential safe and cheaper alternative. It has been demonstrated that SpA is a TNF-α driven disease process. Though the level of this cytokine has been found to be quite high in the synovial and entheseal biopsies, they do not cause commensurate increase in the serum levels. It has been shown that one of the mechanisms of action of conventional DMARDs like SSZ and MTX is by TNF-α blockade. It could be that this benefit is not transmitted to the level of axial and entheseal sites because of the fact that the inflammatory burden in AS is higher. In this setting, a higher dose of the conventional DMARDs may be effective, but this is likely to be associated with significantly increased toxicity profile. The other alternative available is the use of combination DMARD therapy.
Combination DMARD therapy has been tried in rheumatoid arthritis and has been found to be better than monotherapy in halting the clinical and radiological progression of the disease process when given early in the disease [19]. A recent review of the toxicity profile of these agents has proved them to be safe with withdrawal rates due to toxicity being no higher than patients on monotherapy [20]. Considering the effectiveness of combination DMARD therapy in RA, its potential as a safe and cheap alternative for inflammatory Chronic Low Back Ache (CLBA) in SpA needs further investigation.
Most of the studies evaluating the role of DMARDs in SpA, have included patients with advanced disease, in whom significant Ankylosis has already occurred. Damage predominates over disease activity in this cohort and it is often very difficult to distinguish whether symptoms are due to the former or latter. In addition the role of combination therapy in inflammatory CLBA has not been evaluated in well-designed randomized controlled trials.
In this prospective, double blind, placebo-controlled study, we compared the efficacy of SSZ monotherapy versus combination of DMARDs including SSZ, MTX and HCQ, for inflammatory CLBA in relatively early disease of AS/ USpA patients, refractory to NSAID therapy.
Patients who visited our SpA Clinic at Sanjay Gandhi Post- Graduate Institute of Medical Sciences (Lucknow, India), and who fulfilled criteria for the diagnosis of AS by the Modified New York Criteria [21] or USpA by the Amor criteria [22], with disease duration ≤ 8 years, and with inflammatory CLBA of at least 6 months duration were included in the study, if they had a BASDAI ≥ 4 or early morning stiffness ≥ 1 hour despite taking maximum dose of at least one NSAID for 6 weeks duration. The study was carried out between Jan 2010 to Dec 2012.
Patients with renal or hepatic disease, severe uncorrected anemia (Hemoglobin <7 gm/dl), previous exposure to SSZ and/or MTX, pregnant or lactating females, malignancy, chronic or on-going acute infection, were excluded from the study. In addition patients who required and could afford biologicals and those receiving steroids in the previous 3 months were also excluded.
Patients were initially given SSZ 1gm/day which was escalated to 2 g/day after 1 week, and continued until the completion of one month. Patients not tolerating SSZ in the initial month were withdrawn from the study. At the end of the first month, patients were randomized into two groups in a double blind fashion, either Combination DMARD group: MTX (10 mg escalated by 2.5 mg every week up to 20 mg/ week) and HCQS 200 mg/day (MTX + HCQS) or Monotherapy group: placebo MTX and placebo HCQS. SSZ was continued in both the groups for the next 5 months. Randomization sequence was generated by using random digit table. MTX and HCQS and their respective identical looking (shape, color and smell) placebo tablets were first packed in opaque yellow plastic envelops which were then packed inside identical white opaque plastic boxes by another person, who was not a part of the study team. The boxes were coded as box 1xxxA or box 1xxxB and sealed. Box 1xxxA contained either MTX (2.5 mg tablets) or placebo whereas box 1xxxB contained either HCQS or placebo. Both boxes (1xxxA and 1xxxB) provided to a particular patient, contained either only drugs or only placebo. The labeled boxes were distributed to the patients by one of the authors (VA). The key was sealed and stored beyond the reach of the investigators till the completion of the study and data entry, and was opened just before data analysis.
Patients continued their current NSAIDs, and were advised to taper them in accordance with their symptom relief. Patients were required to follow up after completion of 1 month, 2 months, 4 months and 6 months after treatment initiation. Complete hemogram, renal and liver function tests monitored during every visit.
Serum samples for analyzing MMP-3 and TIMP-1 were drawn at baseline and at the end of the study and stored at -80°C till analysis. MMP-3 and TIMP-1 analysis was carried out by ELISA as per the manufacturer recommendations (R&D systems Inc., Minneapolis, MN, USA).
Subject’s written consent was obtained according to the declaration of Helsinki, and study was approved by institutional ethics committee and it conforms to standards currently applied in India. Institutional ethics committee was responsible for data safety and monitoring. All the drugs and matching placebo were procured from IPCA Activa, Mumbai, India.
The primary end point of the study was proportion of patients achieving ASAS 20 response [23] at the end of 6 months. Secondary end points included proportion of patients achieving ASAS 40, changes in the BASDAI [24], BASFI [25], BASMI [26], FACIT [27], patient pain VAS, patient global disease assessment VAS, physician global disease assessment VAS, quality of life measures including the SF-36 [28] and the HAQ at the end of 6 months.
Statistical analysis
Intention to treat analysis was carried out. Patients who did not completed the study; their last observation was carried forward for analysis. Paired T test was used to analyze the numerical data. Mann-Whitney U test and test of proportions was used to calculate the difference between the numbers of patients achieving ASAS20 responses in the combination DMARD vs. SSZ monotherapy group. P value <0.05 was considered significant. All the statistical analysis was carried out on NCSS 2007 software.
Thirty three patients were enrolled in the study with a mean age (24.9 years), M: F sex ratio (10:1), mean disease duration (39 months) and mean BASDAI (6.0). Of these, 27 patients completed the study with 16 being in the combination DMARD group and 11 in the SSZ monotherapy group. Three patients in each group dropped out of the study due to reasons mentioned in the Figure 1.
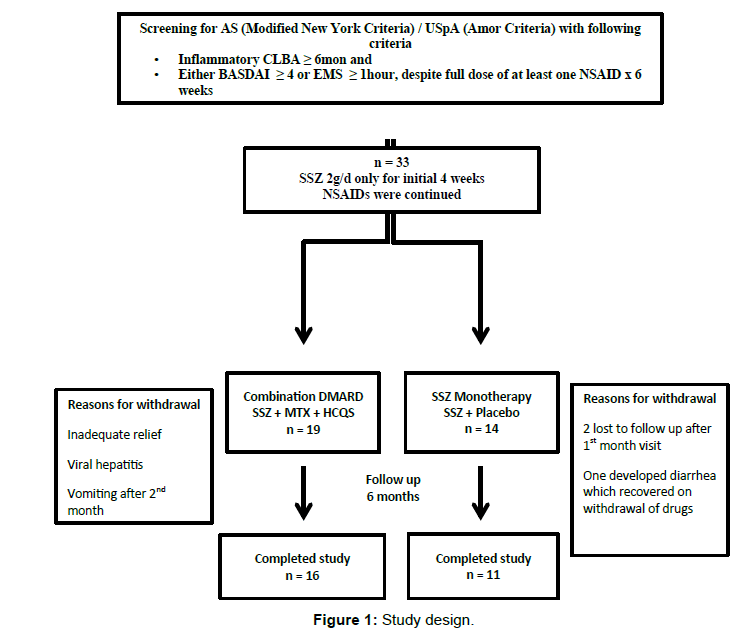
Figure 1: Study design.
Baseline assessments
The baseline characteristics were comparable in both groups (Table 1). The mean age (± S.D) of the patients was 25.4 (± 5.5) and 24.3 (± 4.3) years in the combination DMARD (SSZ+MTX+HCQS) and SSZ monotherapy groups respectively, while the mean duration of disease was 3.1 (± 2.2) and 3.7 (± 1.9) years, respectively. There was one female in each group, with the ratio of patients of AS/USpA being 9/7 (n=16) and 6/5 (n=11) in the combination DMARD group and SSZ monotherapy groups respectively.
| Parameter | Combination DMARD (n = 19) | SSZ Monotherapy (n = 14) | p value |
|---|---|---|---|
| Age (years) | 25.4 ± 5.5 | 24.3 ± 4.3 | 0.55 |
| Gender M:F | 18:1 | 13:1 | NS |
| Duration of CLBA (years) | 3.2 ± 2.3 | 3.7 ± 1.9 | 0.65 |
| No. of AS patients n (%) | 9 (47.3) | 6 (43) | NS |
| No. of USpApatients n (%) | 10 (53.7) | 8 (57) | NS |
| Baseline BASDAI | 6.1 ± 1.3 (4.0 – 9.2) | 5.9 ± 1.5 (4.8 – 8.7) | 0.47 |
| Baseline BASFI | 4.7 ± 2.6 | 5.1 ± 1.8 | 0.81 |
| Baseline BASMI (10 point) | 2.5 ± 1.7 | 2.5 ± 1.5 | 0.86 |
| PGD VAS (0-100) | 59.0 ± 25.1 | 64.1 ± 28.1 | 0.75 |
| Patient Pain VAS (0-100) | 59.9 ± 21.5 | 67.2 ± 27.1 | 0.49 |
| Phy GD VAS (0-100) | 70.2 ± 17.3 | 67.0 ± 9.25 | 0.44 |
| HAQ (0-3) | 1.2 ± 0.6 | 1.5 ± 0.5 | 0.21 |
| FACIT (0-52) | 23.2 ± 9.4 | 28.0 ± 10.4 | 0.36 |
| SF-36 PCS | 33.5 ± 6.6 | 34.8 ± 5.4 | 0.45 |
| SF-36 MCS | 33.8 ± 9.4 | 34.9 ± 9.6 | 0.70 |
*values indicate mean ± SD unless otherwise indicated. Comparison at baseline was done with the Mann-Whitney U test. PGD; Patient global disease, Phy GD; Physician Global Disease
Table 1: Demographic and baseline disease characteristics of the combination DMARD and SSZ monotherapy groups.
Baseline mean BASDAI was 6.1 ± 1.3 (4.0–9.16) and 5.9 ± 1.5 (4.8–8.72) in the combination DMARD and SSZ monotherapy groups, respectively.
Therapy response at the end of 6 months
The primary end point, ASAS 20 response, was achieved in 68.4% (13/19) and 50% (7/14) in the combination DMARD group and the SSZ monotherapy groups (p=0.47, Fisher’s exact test), respectively. BASDAI scores (Table 2) decreased significantly in both the combination DMARD and SSZ monotherapy groups (6.1 ± 1.3[4.0–9.16] to 1.8 ± 1.8[0–5.78] p <0.001; 5.9 ± 1.5[4.8–8.72] to 2.4 ± 1.9[0 – 6.4] p <0.001, respectively). At the completion of 6 months of therapy, BASDAI ≥ 4 was present only in 14.8% (2/16 and 2/11) patients in the combination DMARD and SSZ monotherapy groups, respectively. Other secondary end points (Table 3), including BASFI, patient pain VAS, patient global disease VAS, HAQ, and MCS of SF-36 significantly improved in both the groups, while the 10 point BASMI, FACIT and PCS of SF-36 improved significantly in the combination DMARD group only.
| Parameter | Combination DMARD (n=19) | SSZ monotherapy (n=14) | ||||
|---|---|---|---|---|---|---|
| Baseline | At 6months | p-value | Baseline | At 6months | p-value | |
| BASDAI* | 6.1 ± 1.3 (4.0 – 9.16) | 1.8 ± 1.8 (0 – 5.78) | <0.0001 | 5.9 ± 1.5 (4.8 – 8.72) | 2.4 ± 1.9 (0 – 6.4) | <0.0001 |
| BASDAI ≥ 4.0 n (%) | 19 (100%) | 5 (26.3%) | 14 (100%) | 5 (35.7%) | ||
| BASDAI 50% reduction n (%) | 11 (58%) | 7 (50%) | 0.65 | |||
*Results expressed as mean ± SD (range). Comparison between baseline and 6 month follow up done using paired Student’s t-test. BASDAI 50% reduction analyzed by Chi Square test.
Table 2: BASDAI assessments between the combination DMARD and SSZ monotherapy groups.
| Parameter | Combination DMARD (n = 19) | SSZ monotherapy (n=14) | ||||
|---|---|---|---|---|---|---|
| Baseline | 6 months | p-value | Baseline | 6 months | p-value | |
| BASDAI | 6.1 ± 1.3 | 1.8 ± 1.8 | <0.001 | 5.9 ± 1.5 | 2.4 ± 1.9 | <0.001 |
| BASFI | 4.7 ± 2.6 | 1.3 ± 1.3 | <0.001 | 5.1 ± 1.8 | 2.0 ± 1.7 | 0.001 |
| BASMI 10 point | 2.5 ± 1.7 | 1.9 ± 2.1 | <0.009 | 2.5 ± 1.5 | 2.2 ± 1.7 | 0.291 |
| FACIT (0-52) | 23.2 ± 9.4 | 15.1 ± 11.4 | 0.045 | 28 ± 10.4 | 18.2 ± 11.9 | 0.067 |
| Patient Pain VAS (0-100) | 59.9 ± 21.5 | 19.9 ± 21.6 | <0.001 | 67.2 ± 27.2 | 23.7 ± 18.3 | 0.018 |
| PGD VAS (0-100) | 59.0 ± 25.1 | 19.3 ± 21.0 | <0.001 | 64.1 ± 28.1 | 27.5 ± 22.2 | 0.044 |
| Phy GD VAS (0-100) | 70.2 ± 17.3 | 14.5 ± 11.8 | <0.001 | 67.1 ± 9.3 | 22.3 ± 19.1 | <0.001 |
| PCS | 33.4 ± 6.6 | 44.3 ± 8.8 | <0.001 | 34.8 ± 5.4 | 41.1 ± 6.8 | 0.065 |
| MCS | 33.8 ± 9.4 | 43.4 ± 11.2 | 0.003 | 34.9 ± 9.6 | 44.1 ± 10.7 | 0.028 |
| HAQ (0-3) | 1.2 ± 0.6 | 0.4 ± 0.5 | 0.001 | 1.5 ± 0.5 | 0.5 ± 0.4 | <0.001 |
Table 3: Secondary end points data in the combination DMARD and SSZ monotherapy groups.
The levels of MMP-3 were significantly increased and the levels of TIMP-1 were significantly reduced in the AS/UspA patients as compared to healthy controls at baseline (Table 4). In the Combination DMARD group, the levels of MMP-3 decreased significantly following therapy as compared to the SSZ monotherapy group (Table 5). However, the levels of TIMP-1 remained unchanged in both the groups as compared to baseline.
| AS Patients (n =22) | Healthy Control (n= 20) | P value | |
|---|---|---|---|
| MMP 3 | 48.29 ± 14.92 | 13.34 ± 5.48 | <0.001 |
| TIMP-1 | 132.76 ± 32.58 | 181.05 ± 19.10 | <0.001 |
Results expressed in ng/ml
Table 4: Serum levels of MMP3 and TIMP-1 in AS patients and healthy controls.
| Parameter | Drug (n = 15) | Placebo (n = 7) | ||||
|---|---|---|---|---|---|---|
| Baseline | Follow-up | p value | Baseline | Follow-up | p value | |
| MMP 3 | 45.0 ± 15.3 | 30.4 ± 17.6 | 0.001 | 55.4 ± 12.0 | 53.8 ± 9.2 | 0.756 |
| TIMP-1 | 137.1 ± 37.2 | 131.4 ± 30.1 | 0.271 | 123.5 ± 18.5 | 121.7 ± 34.4 | 0.809 |
(Results are expressed in ng/ml).
Table 5: Effect of combination DMARD vs. SSZ monotherapy on serum levels of MMP 3 and TIMP-1.
Toxicity profile
Almost all patients tolerated the drugs except for one patient in the SSZ monotherapy group who withdrew due to drug induced diarrhea, which recovered after stopping the drug, and one patient in the combination DMARD group who developed drug associated vomiting after which he withdrew at the end of 2 months. One patient developed transient transamniitis which required discontinuation of medications for 4 weeks but patient completed the study without recurrence.
In this prospective, double-blind, placebo-controlled study, we have assessed the efficacy of combination DMARDs (SSZ+MTX+HCQS) versus that of SSZ monotherapy in NSAID refractory inflammatory CLBA in patients with AS/ USpA of relatively short duration (≤ 8 years). The disease duration chosen was based on an Indian study which showed that the average delay from the onset of initial symptoms to diagnosis was 8 years [29].
In the present study we observed that both combination DMARD as well as SSZ monotherapy are effective in the treatment of NSAID refractory inflammatory CLBA in SpA of short disease duration. We found that combination of MTX, HCQS and SSZ, did not provide additional efficacy over that provided by SSZ monotherapy, as evidenced by the ASAS 20 responses of 68% (13/19) and 50% (7/14) in the two groups respectively. BASDAI improved significantly in both the groups compared to baseline, and at the end of 6 months all but 4 (14.8%) patients had a BASDAI <4. Both the therapies were well tolerated.
DMARDs for axial symptomatology in SpA, have been evaluated in a very limited number of studies. Although SSZ is the most well evaluated of these, its efficacy is mostly limited to peripheral arthritis associated with SpA [6]. The ASCEND trial, which compared Etanercept 50 mg once weekly with SSZ 3g/d for 16 weeks, in active AS with both axial and peripheral symptoms, reported that ASAS 20 responses were achieved in almost 52.9% on SSZ, which is a significant number, though it was inferior to Etanercept (75.9%; p<0.0001). The mean disease duration in the study was 7.6 years [30]. The study by Braun et al., evaluating SSZ vs. placebo in inflammatory CLBA associated with AS/ USpA, included 230 patients, with 47% also having peripheral arthritis. At the end of 6 months, there was no significant difference in the reduction in BASDAI and most other secondary outcome variables between the two groups, though in the group without peripheral arthritis, there was significant benefit with SSZ in reduction in BASDAI, spinal pain and morning stiffness compared to placebo [8]. In a re-analysis of three randomized, placebo controlled trials of SSZ 2g/day vs. placebo in AS, PsA and ReA by the Department of Veterans Affairs Cooperative Study group, SSZ was found to be effective in peripheral articular manifestations, but not in axial disease [7].
In a retrospective study on the efficacy of combination DMARDs (SSZ + MTX) versus SSZ monotherapy in NSAID refractory AS, Can et al. had reported a significant improvement in BASDAI scores in both the groups at 6 months, which consequently lead to a reduction in the requirement of biological therapy by 21-24% if BASDAI was the decisive factor. BASDAI was >4 in 32.8% (20/61) of patients in the SSZ monotherapy and in 44% (11/26) in the combination arm at the end of 6 month follow up [31]. This being a retrospective study is obviously biased by the physicians’ subjectivity in disease assessment and their personal choices with regards to therapy.
To the best of our knowledge, this is the first placebo controlled double blind study, to evaluate the efficacy of combination DMARDs, which includes the combination of SSZ + MTX + HCQ, for inflammatory CLBA in AS/USpA. In addition we have included patients with relatively shorter disease duration, which ensures a more precise assessment of disease activity, and hence partially obviating the influence of damage in assessment of disease activity. In the present study we have observed that both combination DMARDs and SSZ monotherapy are associated with good response to treatment in SpA patient with NSAID refractory inflammatory CLBA. Though superiority (as far as ASAS20 response is considered) of combination of MTX, HCQS and SSZ was not observed however, combination DMARD group has significant improvement in physical component score of SF-36, BASMI and fatigue as compared to SSZ monotherapy group. Moreover, more number of patients reported ASAS 20 responses in the combination DMARD group. May be due to small number of patients in both the groups the study was not sufficiently powered to demonstrate superiority of combination DMARD therapy as compared to SSZ monotherapy group.
MMP-3 has been reported to reflect degree of inflammation [32] and correlate with disease activity in AS [33] and radiographic progression [34]. MMP-3 is involved in degradation of extracellular matrix proteins and is involved in degradation of cartilage and bone of inflamed joints [35]. We observed significant decrease in MMP-3 levels in the combination DMARD group as compared to SSZ monotherapy group. Thus combination DMARD therapy has potential to minimize joint damage by reducing the levels of MMP-3.
The limitations of our study include the small sample size due to single center and rigid inclusion criteria and absence of a control arm with only NSAIDs, due to its perceived unethicality in a cohort which is already in discomfort due to NSAID refractoriness.
Hence we conclude that, in a small cohort of patients SSZ monotherapy is efficacious in a significant proportion of patients with NSAID refractory, inflammatory CLBA associated with AS/ USpA in relatively early disease, and would help probably delay or may be totally avoid the use of expensive anti-TNF biologics and its associated complications in this subset, especially in the under developed world. Moreover, we have found that the triple combination of SSZ, MTX and HCQS is not superior to SSZ monotherapy. However, a larger study with sufficient sample size and power is necessary to make a definite recommendation.
Authors acknowledge the support of IPCA Activa, Mumbai, India for their generous support in supplying the study drugs as well as placebo.
