Case Report - (2017) Volume 3, Issue 3
Introduction: We present the case of a 20-year-old male with a pure yolk sac tumor in the right testicle and metastatic disease to liver, retroperitoneum, and lung; with an evolution of approximately three months from diagnosis to death.
Materials and methods: Case report and literature review.
Conclusion: Pure yolk sac testicular tumor in an adult is extremely uncommon. The adult presentation has a more aggressive biological behavior. There is still controversy regarding the treatment, more research is needed to define the optimal management.
Keywords: Cancer of the Testes; Endodermal sinus tumor; Yolk sac tumor; Orchiectomy; Adult; Metastasis; Germ cell tumor
Testicular cancer is the most common malignant neoplasm in men between the ages of 15 and 35, although it accounts for only 1% of male malignancies [1]. 95% originated from germ cells, which are the main cell type of the testis, and more than half of the germinal tumors contain a mixture of multiple histological types, forming mixed entities [2,3].
Germ Cell Tumors (GCT) occur at all ages, and there are clearly identified risk factors, including: congenital genital malformations such as: undescended testis, family history of testicular tumors in first-degree relatives (father and siblings, 6 and 10 times more risk respectively), presence of contralateral tumor, infertility and exposure to diethylstilbestrol [4].
The yolk sac tumor (YST), also known as endodermal sinus tumor, is the most common GCT in infants and children, accounting for 80% of germ cell tumors in this age group [5]. It is observed only in 2.4% of adult patients in their pure form since up to 42% of mixed GCTs have some component of the yolk sac [6].
Due to the unusual presentation of the YST beyond de pediatric age (there are less than ten cases reported in the literature) there is no consensus in therapy after radical orchiectomy.
We present the case of a 20-year-old male with a pure YST in the right testicle, metastatic to liver, retroperitoneum, and lung; with an evolution of approximately three months from diagnosis to death.
A previously healthy 20-year-old man, consulted to the emergency department for two days of emesis and abdominal pain associated with jaundice.
On physical exam, the patient was stable, conscious and icteric. He had a distended abdomen, painful on palpation, but without signs of peritoneal irritation.
Laboratory findings showed pancreatic amylase and hepatic transaminases were high. The CT scan of the abdomen showed a hypodense image in the pancreas head and duodenum, as well as a hepatic and retroperitoneal mass with thickening of the mesentery and pleural effusion.
Based on the previous history, the initial diagnosis was an abdominal sepsis secondary to severe acute necrotizing obstructive pancreatitis by an extrinsic compression of a large retroperitoneal mass. The patient was admitted to the intensive care unit, in which interventional radiology drained the peripancreatic collection and took a biopsy of the retroperitoneal mass.
Given the severity of the clinical presentation, laboratory findings and physical examination, the diagnostic and therapeutic efforts were initially focused on the diagnosis of acute pancreatitis.
On the second day in intensive care unit, physical examination revealed a large right testicular mass, not painful on palpation. Testicular ultrasonography reported a mass of 10 × 10 centimeters of heterogeneous echogenicity, predominantly hypoechoic, with cystic areas and images of microcalcifications. After this crucial finding, the patient mentioned a two-weeks history of non-painful, fast-growing, non-traumatic testicular mass.
In the urological evaluation, all three serum tumoral markers were high: hCG (10.896 mUI/mL), AFP (20.000 ng/mL) and LDH (2.188 U/l). Right radical orchiectomy was performed without complications (Figures 1 and 2).
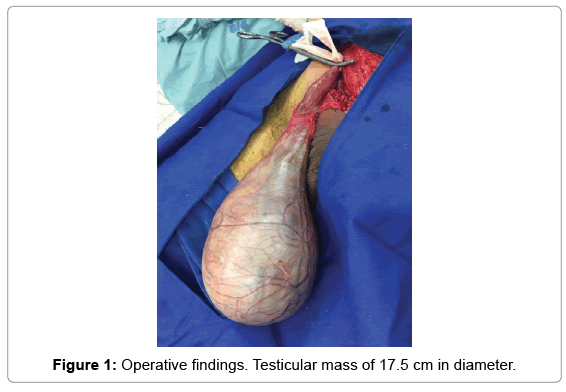
Figure 1: Operative findings. Testicular mass of 17.5 cm in diameter.
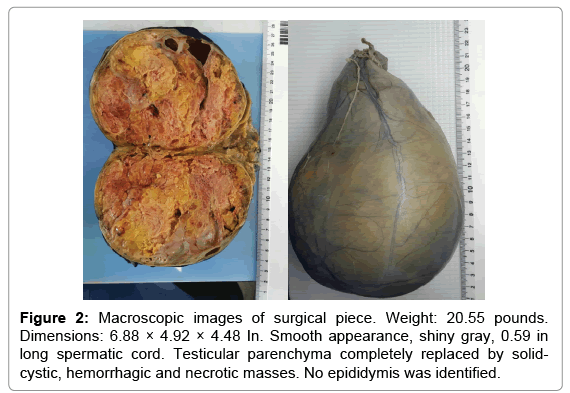
Figure 2: Macroscopic images of surgical piece. Weight: 20.55 pounds. Dimensions: 6.88 × 4.92 × 4.48 In. Smooth appearance, shiny gray, 0.59 in long spermatic cord. Testicular parenchyma completely replaced by solidcystic, hemorrhagic and necrotic masses. No epididymis was identified.
The histopathological analysis of the specimen showed a nonseminomatous germ cell tumor, being the yolk sac the only tumoral component identified (Figures 3 and 4). (Immunohistochemistry, tumoral cells: positivity for Alfaprotein, Negativity for CD30, PLAP, OCT 3/4 and CKIT).
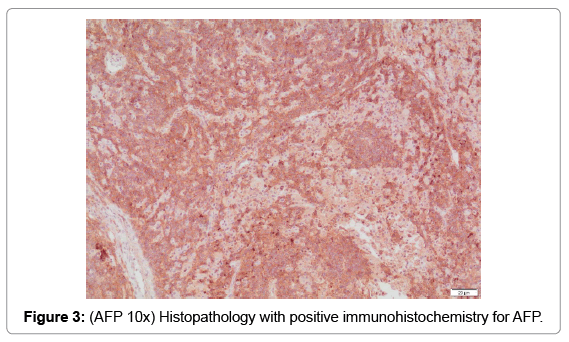
Figure 3: (AFP 10x) Histopathology with positive immunohistochemistry for AFP.
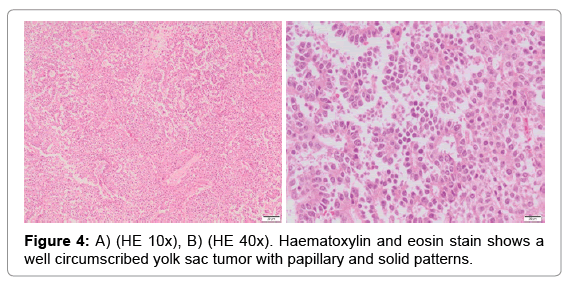
Figure 4: A) (HE 10x), B) (HE 40x). Haematoxylin and eosin stain shows a well circumscribed yolk sac tumor with papillary and solid patterns.
After the orchiectomy, the plan was initiate chemotherapy with curative intention, once the infection was resolved, however, the patient had a torpid evolution, with poor modulation of inflammatory response. Three months after the hospitalization the patient died from a ventilatory failure, without even initiating the first chemotherapy cycle.
The YST is characterized by the presence of tissue that resembles the yolk sac, allantois or extraembryonic mesenchyme [6].
Yolk sac tumors occurs in men and women, in the testis, ovary, and other sites, such as the mediastinum [7]. In the testis, the presentation is divided into 2 age groups: i) pure YST, typically observed in children and ii) YST as a component of a mixed tumor in adults (the pure form in an adult patient is extremely unusual) (Table 1).
| Histological subtypesof testicular tumors | Frequency |
|---|---|
| Seminoma | 26.9% |
| Tumors of non-seminomatous germinal cells | |
| Embryonal carcinoma | 3.1% |
| Coriocarcinoma | 0.1% |
| Yolk sac/Endodermal sinus tumor | 2.4% |
| Teratoma | 2.7% |
| Mixed tumors | 60% |
| Spermatocytictumor | 2.4% |
Table 1: Frequency and histological subtypes of testicular tumors in adults. Source: Adapted from tumours of the urinary system and male genital organs. Moch H, Humphrey PA, Ulbright TM, et al (eds). In: World Health Organization Classification of Tumours. Lyon. 2016.
Pure YST is the most common testicular neoplasm in prepubertal children, accounting for 80% of testicular GCT in this group, with a mean age of presentation of 1.5 years, on the other side, in adults it is present as a component of mixed non-seminomatous germ cell tumor, with an average age of 25-30 years [8].
The immunohistochemistry analysis will determine the composition of the testicular tumor. YST are positive for AFP (single chain glycoprotein that is normally secreted during fetal development by the yolk sac, liver and gastrointestinal tract) in 90% of cases [9], therefore, the absence of AFP in immunohistochemistry does not exclude the diagnosis of YST.
Microscopically, there are more than 10 different subtypes described papillary, reticular, glandular, solid, hepatoid, glanduloalveolar, polypsicular vitelline, myxomatous, among others [10,11]. None of these modalities differ in prognostic value.
In general, testicular tumors appear as painless masses, which are typically bulky, slow-growing, progressive lesions. On the other hand, in advanced metastatic disease, the symptoms may be unclear or associated with compromise of the organs affected by the tumor dissemination, which makes the diagnosis difficult and delayed. In addition, the patient may undergo unnecessary interventions and studies that further prolong the diagnostic window.
Regarding treatment, it should be noted that because of the low incidence, there is no therapeutic consensus beyond radical orchiectomy [6,10] and the options are limited by tumor progression at the time of diagnosis.
Non-seminomatous tumors in the advanced stages (IIC and III) are considered to be poor prognosis when associated with any of the following criteria: visceral metastases, AFP>10.000 ng/ml, HCG>50.000 IU/l or LDH>10 × ULN [12]. Belong to this category implies a 5-year survival rate of less than 48%, very low considering that the presentation of this tumors usually occurs at early age. Therefore, the guidelines recommend the referral of these patients to specialized cancer centers to continue follow-up.
As an adjuvant treatment, 4 chemotherapy cycles can be performed initially with cisplatin, etoposide or ifosfamide; however, 5-year progression-free survival is between 45% to 50% in patients with favorable response to the first cycles (decrease in serum tumor markers). Otherwise, there is no general recommendation; one of the possibilities is to continue the scheme at low doses to reduce the risk of sudden death [12,13].
Germ cell tumors are a heterogeneous group of neoplasms, both in their histology and in the clinical course. Pure yolk sac testicular tumor in the adult is an unusual clinical entity and it is relevant for its greater biological aggressiveness. The literature data do not count with larges series of patients and, there is no consensus regarding the management after radical orchiectomy.
Nowadays, thanks to the rapid advancement of technology and diagnostic methods, the relevance of performing a complete medical history and a detailed physical examination, key to an early diagnosis, has been lost. In this case, it is crucial to emphasize the importance of genital examination in every young man, which in many cases is left aside by non-urologists physicians in different specialties.
Thanks to Eugenio Meek B. MD, pathologist at the San Ignacio University Hospital, for the analysis of the surgical specimen and the interpretation of histological slides.